

Form 8-K Silverback Therapeutics, For: Sep 16
 Tweet
Tweet Share
Share

Exhibit 99.1Exhibit 99.1

Forward-looking statements and disclaimers Any reproduction or distribution of this presentation, in whole or in part, or the disclosure of any of its contents is prohibited. This presentation includes certain forward-looking statements that involve risks and uncertainties that could cause actual results to be materially different from historical results or from any future results expressed or implied by such forward-looking statements regarding Silverback Therapeutics, Inc. (the “Company”). These forward-looking statement include, but are not limited to, those regarding the Company’s plans and ability to bring new treatments to patients in need, including potential combination efforts, the progress and expected timing of the Company’s drug development programs and clinical trials, clinical development plans and timelines, regulatory matters, market size and opportunity, the Company’s future financial position, the Company’s strategy and intellectual property matters, and Company estimates regarding expenses, capital requirements, and needs for additional financing. These forward-looking statements are based on the beliefs of the Company’s management as well as assumptions made and information currently available to the Company. Such statements reflect the current views of the Company with respect to future events and are subject to business, regulatory, economic and competitive risks, uncertainties, contingencies and assumptions about the Company, including, among other things, the development of its business, trends in the industry, the legal and regulatory framework for the industry, and future expenditures. Factors that may cause actual results to differ materially include the risk that compounds that appeared promising in early research or clinical trials do not demonstrate safety and/or efficacy in later preclinical studies or clinical trials, the risk that the Company may not obtain approval to market its product candidates, uncertainties associated with performing clinical trials, regulatory filings and applications, risks associated with reliance on third parties to successfully conduct clinical trials, the risks associated with reliance on outside financing to meet capital requirements, and other risks associated with the process of discovering, developing and commercializing drugs that are safe and effective for use as human therapeutics, and in the endeavor of building a business around such drugs. In light of these risks, uncertainties, contingencies and assumptions, the events or circumstances referred to in the forward-looking statements may not occur. None of the future projections, expectations, estimates or prospects in this presentation should be taken as forecasts or promises nor should they be taken as implying any indication, assurance or guarantee that the assumptions on which such future projections, expectations, estimates or prospects have been prepared are correct or exhaustive or, in the case of the assumptions, fully stated in the presentation. The actual results may vary from the anticipated results and the variations may be material. You are urged to consider statements that include the words may, will, would, could, should, believes, estimates, projects, promise, potential, expects, plans, anticipates, intends, continues, designed, goal, or the negative of those words or other comparable words to be uncertain and forward-looking. For a further list and description of the risks and uncertainties that the Company faces, please refer to the Company’s periodic and other filings with the Securities and Exchange Commission, which are available at www.sec.gov. Such forward-looking statements are current only as of the date they are made, and the Company assumes no obligation to update any forward-looking statements, whether as a result of new information, future events, or otherwise. This presentation discusses product candidates that are under clinical study and which have not yet been approved for marketing by the U.S. Food and Drug Administration. No representation is made as to the safety or effectiveness of these product candidates for the use for which such product candidates are being studied. The trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of such products. 2Forward-looking statements and disclaimers Any reproduction or distribution of this presentation, in whole or in part, or the disclosure of any of its contents is prohibited. This presentation includes certain forward-looking statements that involve risks and uncertainties that could cause actual results to be materially different from historical results or from any future results expressed or implied by such forward-looking statements regarding Silverback Therapeutics, Inc. (the “Company”). These forward-looking statement include, but are not limited to, those regarding the Company’s plans and ability to bring new treatments to patients in need, including potential combination efforts, the progress and expected timing of the Company’s drug development programs and clinical trials, clinical development plans and timelines, regulatory matters, market size and opportunity, the Company’s future financial position, the Company’s strategy and intellectual property matters, and Company estimates regarding expenses, capital requirements, and needs for additional financing. These forward-looking statements are based on the beliefs of the Company’s management as well as assumptions made and information currently available to the Company. Such statements reflect the current views of the Company with respect to future events and are subject to business, regulatory, economic and competitive risks, uncertainties, contingencies and assumptions about the Company, including, among other things, the development of its business, trends in the industry, the legal and regulatory framework for the industry, and future expenditures. Factors that may cause actual results to differ materially include the risk that compounds that appeared promising in early research or clinical trials do not demonstrate safety and/or efficacy in later preclinical studies or clinical trials, the risk that the Company may not obtain approval to market its product candidates, uncertainties associated with performing clinical trials, regulatory filings and applications, risks associated with reliance on third parties to successfully conduct clinical trials, the risks associated with reliance on outside financing to meet capital requirements, and other risks associated with the process of discovering, developing and commercializing drugs that are safe and effective for use as human therapeutics, and in the endeavor of building a business around such drugs. In light of these risks, uncertainties, contingencies and assumptions, the events or circumstances referred to in the forward-looking statements may not occur. None of the future projections, expectations, estimates or prospects in this presentation should be taken as forecasts or promises nor should they be taken as implying any indication, assurance or guarantee that the assumptions on which such future projections, expectations, estimates or prospects have been prepared are correct or exhaustive or, in the case of the assumptions, fully stated in the presentation. The actual results may vary from the anticipated results and the variations may be material. You are urged to consider statements that include the words may, will, would, could, should, believes, estimates, projects, promise, potential, expects, plans, anticipates, intends, continues, designed, goal, or the negative of those words or other comparable words to be uncertain and forward-looking. For a further list and description of the risks and uncertainties that the Company faces, please refer to the Company’s periodic and other filings with the Securities and Exchange Commission, which are available at www.sec.gov. Such forward-looking statements are current only as of the date they are made, and the Company assumes no obligation to update any forward-looking statements, whether as a result of new information, future events, or otherwise. This presentation discusses product candidates that are under clinical study and which have not yet been approved for marketing by the U.S. Food and Drug Administration. No representation is made as to the safety or effectiveness of these product candidates for the use for which such product candidates are being studied. The trademarks included herein are the property of the owners thereof and are used for reference purposes only. Such use should not be construed as an endorsement of such products. 2
Corporate highlights ImmunoTAC conjugates are designed to unlock a new class of targeted immuno-oncology agents that direct a 1 myeloid cell agonist to the tumor microenvironment for localized activation Emerging clinical data supports proof-of-mechanism for localized TLR8 agonism and the ImmunoTAC platform, 2 evidenced by the robust activation of innate and adaptive immune response seen in patients SBT6050 has demonstrated early signals of anti-tumor activity as a monotherapy and in combination with a 3 PD-1 inhibitor, with a manageable safety profile consistent with an active IO agent Clinical development plan to evaluate SBT6050 in combinations designed to have long-term benefit in early lines 4 of treatment, including combo with anti-PD1, with Enhertu and with Herceptin/Tukysa Positive readthrough to Silverback’s TLR8 pipeline with value-generating milestones expected in the next 6-18 5 months, including anticipated initiation of SBT6290 (Nectin4) Ph1 study and SBT8230 (HBV) Ph1-enabling studies 3Corporate highlights ImmunoTAC conjugates are designed to unlock a new class of targeted immuno-oncology agents that direct a 1 myeloid cell agonist to the tumor microenvironment for localized activation Emerging clinical data supports proof-of-mechanism for localized TLR8 agonism and the ImmunoTAC platform, 2 evidenced by the robust activation of innate and adaptive immune response seen in patients SBT6050 has demonstrated early signals of anti-tumor activity as a monotherapy and in combination with a 3 PD-1 inhibitor, with a manageable safety profile consistent with an active IO agent Clinical development plan to evaluate SBT6050 in combinations designed to have long-term benefit in early lines 4 of treatment, including combo with anti-PD1, with Enhertu and with Herceptin/Tukysa Positive readthrough to Silverback’s TLR8 pipeline with value-generating milestones expected in the next 6-18 5 months, including anticipated initiation of SBT6290 (Nectin4) Ph1 study and SBT8230 (HBV) Ph1-enabling studies 3
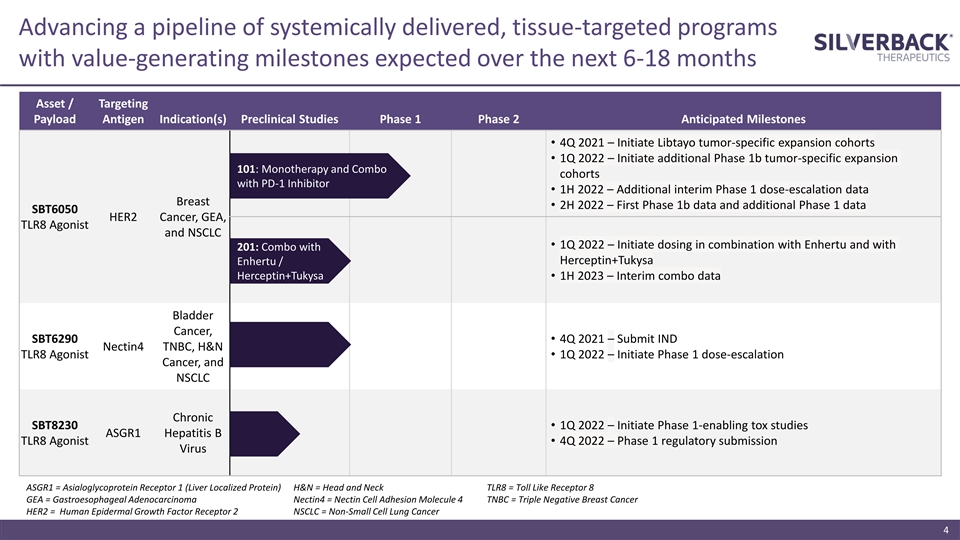
Advancing a pipeline of systemically delivered, tissue-targeted programs with value-generating milestones expected over the next 6-18 months Asset / Targeting Payload Antigen Indication(s) Preclinical Studies Phase 1 Phase 2 Anticipated Milestones • 4Q 2021 – Initiate Libtayo tumor-specific expansion cohorts • 1Q 2022 – Initiate additional Phase 1b tumor-specific expansion 101: Monotherapy and Combo cohorts with PD-1 Inhibitor • 1H 2022 – Additional interim Phase 1 dose-escalation data Breast • 2H 2022 – First Phase 1b data and additional Phase 1 data SBT6050 HER2 Cancer, GEA, TLR8 Agonist and NSCLC • 1Q 2022 – Initiate dosing in combination with Enhertu and with 201: Combo with Herceptin+Tukysa Enhertu / Herceptin+Tukysa• 1H 2023 – Interim combo data Bladder Cancer, SBT6290• 4Q 2021 – Submit IND Nectin4 TNBC, H&N TLR8 Agonist• 1Q 2022 – Initiate Phase 1 dose-escalation Cancer, and NSCLC Chronic SBT8230• 1Q 2022 – Initiate Phase 1-enabling tox studies ASGR1 Hepatitis B TLR8 Agonist• 4Q 2022 – Phase 1 regulatory submission Virus ASGR1 = Asialoglycoprotein Receptor 1 (Liver Localized Protein) H&N = Head and Neck TLR8 = Toll Like Receptor 8 GEA = Gastroesophageal Adenocarcinoma Nectin4 = Nectin Cell Adhesion Molecule 4 TNBC = Triple Negative Breast Cancer HER2 = Human Epidermal Growth Factor Receptor 2 NSCLC = Non-Small Cell Lung Cancer 4Advancing a pipeline of systemically delivered, tissue-targeted programs with value-generating milestones expected over the next 6-18 months Asset / Targeting Payload Antigen Indication(s) Preclinical Studies Phase 1 Phase 2 Anticipated Milestones • 4Q 2021 – Initiate Libtayo tumor-specific expansion cohorts • 1Q 2022 – Initiate additional Phase 1b tumor-specific expansion 101: Monotherapy and Combo cohorts with PD-1 Inhibitor • 1H 2022 – Additional interim Phase 1 dose-escalation data Breast • 2H 2022 – First Phase 1b data and additional Phase 1 data SBT6050 HER2 Cancer, GEA, TLR8 Agonist and NSCLC • 1Q 2022 – Initiate dosing in combination with Enhertu and with 201: Combo with Herceptin+Tukysa Enhertu / Herceptin+Tukysa• 1H 2023 – Interim combo data Bladder Cancer, SBT6290• 4Q 2021 – Submit IND Nectin4 TNBC, H&N TLR8 Agonist• 1Q 2022 – Initiate Phase 1 dose-escalation Cancer, and NSCLC Chronic SBT8230• 1Q 2022 – Initiate Phase 1-enabling tox studies ASGR1 Hepatitis B TLR8 Agonist• 4Q 2022 – Phase 1 regulatory submission Virus ASGR1 = Asialoglycoprotein Receptor 1 (Liver Localized Protein) H&N = Head and Neck TLR8 = Toll Like Receptor 8 GEA = Gastroesophageal Adenocarcinoma Nectin4 = Nectin Cell Adhesion Molecule 4 TNBC = Triple Negative Breast Cancer HER2 = Human Epidermal Growth Factor Receptor 2 NSCLC = Non-Small Cell Lung Cancer 4

ImmunoTAC platform strategically pairs antigen binding domains with linker-payloads to modulate pathways underlying serious diseases Library of Proprietary Molecules Antigen Binding Domains Antigen binding domain HER2 Nectin4 ASGR1 Undisclosed Linker-payload Linker-Payloads Fc region TLR8 TGFbR Undisclosed Agonist Antagonist Robust IP portfolio with 4 issued patents and over 100 patent applications pending worldwide directed to payloads, conjugates, and antibodies, for use in cancer, virology and fibrosis 5ImmunoTAC platform strategically pairs antigen binding domains with linker-payloads to modulate pathways underlying serious diseases Library of Proprietary Molecules Antigen Binding Domains Antigen binding domain HER2 Nectin4 ASGR1 Undisclosed Linker-payload Linker-Payloads Fc region TLR8 TGFbR Undisclosed Agonist Antagonist Robust IP portfolio with 4 issued patents and over 100 patent applications pending worldwide directed to payloads, conjugates, and antibodies, for use in cancer, virology and fibrosis 5
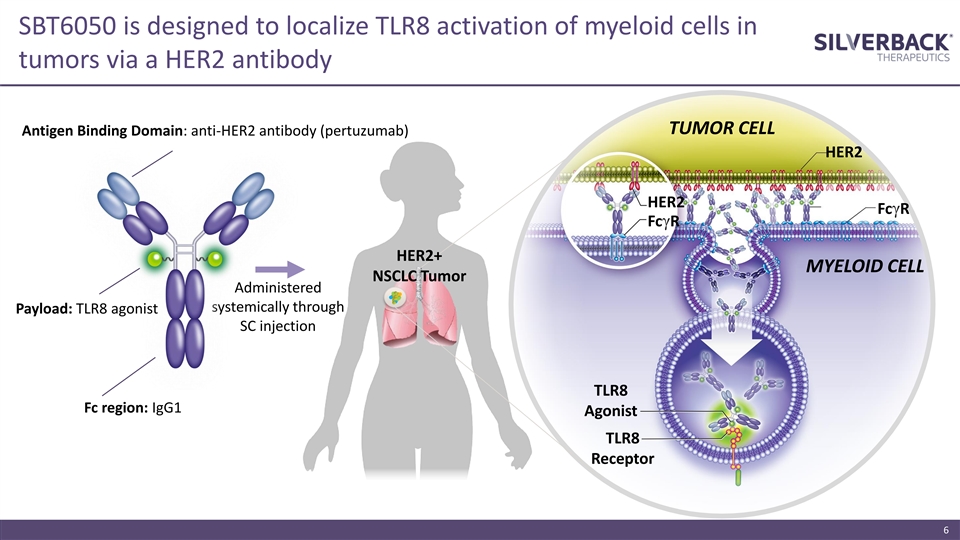
SBT6050 is designed to localize TLR8 activation of myeloid cells in tumors via a HER2 antibody TUMOR CELL Antigen Binding Domain: anti-HER2 antibody (pertuzumab) HER2 HER2 FcγR FcγR HER2+ MYELOID CELL NSCLC Tumor Administered systemically through Payload: TLR8 agonist SC injection TLR8 Fc region: IgG1 Agonist TLR8 Receptor 6SBT6050 is designed to localize TLR8 activation of myeloid cells in tumors via a HER2 antibody TUMOR CELL Antigen Binding Domain: anti-HER2 antibody (pertuzumab) HER2 HER2 FcγR FcγR HER2+ MYELOID CELL NSCLC Tumor Administered systemically through Payload: TLR8 agonist SC injection TLR8 Fc region: IgG1 Agonist TLR8 Receptor 6

TLR8 is highly expressed in human myeloid cell types that elicit anti-tumor responses when activated TLR8 Agonism Direct Effects Indirect Effects Macrophages Dendritic Cells Myeloid Derived Monocytes NK Cells T Cells B Cells Suppressor Cells Direct tumor killing Promote anti-tumor Reprogramming to a Immune cell Direct tumor killing Direct tumor killing Antigen Pro-inflammatory T cell responses and pro-inflammatory recruitment Creation of a pro- presentation environment infiltration state Tumor killing and inflammatory Activate T cells Immune cell stimulation environment Produce antibodies recruitment Myeloid cells can comprise between 5-10% of the tumor, at least twice the prevalence of T cells* * Zhang et al, Journal of Cancer 2019 7TLR8 is highly expressed in human myeloid cell types that elicit anti-tumor responses when activated TLR8 Agonism Direct Effects Indirect Effects Macrophages Dendritic Cells Myeloid Derived Monocytes NK Cells T Cells B Cells Suppressor Cells Direct tumor killing Promote anti-tumor Reprogramming to a Immune cell Direct tumor killing Direct tumor killing Antigen Pro-inflammatory T cell responses and pro-inflammatory recruitment Creation of a pro- presentation environment infiltration state Tumor killing and inflammatory Activate T cells Immune cell stimulation environment Produce antibodies recruitment Myeloid cells can comprise between 5-10% of the tumor, at least twice the prevalence of T cells* * Zhang et al, Journal of Cancer 2019 7

Proof-of-mechanism established in 40 patient dose escalation study* SBT6050 ▪ Pharmacodynamic (PD) markers indicative of myeloid and T/NK cell activation generally increase with dose, plateauing at 0.6 mg/kg ▪ PD activity is maintained with repeat dosing ▪ SBT6050 payload detected in intratumoral macrophages and on tumor cells SBT6050 monotherapy or in combo with pembro has a manageable safety profile ▪ Common adverse events consistent with immune activation ▪ Safety profile of SBT6050 in combination with pembrolizumab was similar to SBT6050 monotherapy ▪ Non-overlapping adverse events with other HER2-directed agents support combination with Enhertu and Herceptin+Tukysa Tumor-localizing antigen: HER2 moderate and high expression (pertuzumab epitope targeted) Early signals of anti-tumor activity in a heavily pre-treated heterogenous population ▪ Among 18 evaluable patients for tumor types of interest, one Partial Response (PR) Target cell: myeloid cells (-55%, NSCLC) maintained at the most recent available scan obtained at 36 weeks post-enrollment, and 8 weeks after discontinuing study treatment Payload: proprietary TLR8 agonist ▪ Stable Disease (SD) reported in seven patients Next readout: 1H 2022 – additional interim Phase 1 dose-escalation data * August 1, 2021 data cut-off date 8Proof-of-mechanism established in 40 patient dose escalation study* SBT6050 ▪ Pharmacodynamic (PD) markers indicative of myeloid and T/NK cell activation generally increase with dose, plateauing at 0.6 mg/kg ▪ PD activity is maintained with repeat dosing ▪ SBT6050 payload detected in intratumoral macrophages and on tumor cells SBT6050 monotherapy or in combo with pembro has a manageable safety profile ▪ Common adverse events consistent with immune activation ▪ Safety profile of SBT6050 in combination with pembrolizumab was similar to SBT6050 monotherapy ▪ Non-overlapping adverse events with other HER2-directed agents support combination with Enhertu and Herceptin+Tukysa Tumor-localizing antigen: HER2 moderate and high expression (pertuzumab epitope targeted) Early signals of anti-tumor activity in a heavily pre-treated heterogenous population ▪ Among 18 evaluable patients for tumor types of interest, one Partial Response (PR) Target cell: myeloid cells (-55%, NSCLC) maintained at the most recent available scan obtained at 36 weeks post-enrollment, and 8 weeks after discontinuing study treatment Payload: proprietary TLR8 agonist ▪ Stable Disease (SD) reported in seven patients Next readout: 1H 2022 – additional interim Phase 1 dose-escalation data * August 1, 2021 data cut-off date 8

Phase 1/1b dose escalation study; projected RP2D determined for expansion cohorts Part 1: monotherapy dose escalation Part 2: monotherapy tumor specific cohorts SBT6050 SC injection Q2W SBT6050 SC injection Q2W HER2-expressing (IHC 2+ or 3+) or HER2-amplified advanced cancers expressing HER2 BC, gastric/GEJ, and NSCLC 0.3 mg/kg 0.6 mg/kg 0.9 mg/kg 1.2 mg/kg Part 3: pembrolizumab combination dose escalation Part 4: pembrolizumab combination expansion cohort HER2-expressing (IHC 2+ or 3+) or HER2-amplified advanced cancers SBT6050 SC injection Q2W; pembrolizumab 400 mg IV Q6W SBT6050 SC injection Q2W; pembrolizumab 400 mg IV Q6W expressing HER2 solid tumors 0.15 mg/kg 0.3 mg/kg 0.6 mg/kg* Part 5: cemiplimab combination expansion cohort SBT6050 SC injection Q3W; cemiplimab 350 mg/kg IV Q3W positive expressing HER2 gastric/GEJ cancer, HER2 NSCLC HER2 status: positive HER2 = HER2 IHC 3+ or IHC 2+/amplified expressing HER2 = HER2 IHC 2+, or IHC3+, or amplified low HER2 = HER2 IHC 2+/ not amplified *Currently enrolling | Data presented are interim data with a data cut-off date of August 1, 2021 9Phase 1/1b dose escalation study; projected RP2D determined for expansion cohorts Part 1: monotherapy dose escalation Part 2: monotherapy tumor specific cohorts SBT6050 SC injection Q2W SBT6050 SC injection Q2W HER2-expressing (IHC 2+ or 3+) or HER2-amplified advanced cancers expressing HER2 BC, gastric/GEJ, and NSCLC 0.3 mg/kg 0.6 mg/kg 0.9 mg/kg 1.2 mg/kg Part 3: pembrolizumab combination dose escalation Part 4: pembrolizumab combination expansion cohort HER2-expressing (IHC 2+ or 3+) or HER2-amplified advanced cancers SBT6050 SC injection Q2W; pembrolizumab 400 mg IV Q6W SBT6050 SC injection Q2W; pembrolizumab 400 mg IV Q6W expressing HER2 solid tumors 0.15 mg/kg 0.3 mg/kg 0.6 mg/kg* Part 5: cemiplimab combination expansion cohort SBT6050 SC injection Q3W; cemiplimab 350 mg/kg IV Q3W positive expressing HER2 gastric/GEJ cancer, HER2 NSCLC HER2 status: positive HER2 = HER2 IHC 3+ or IHC 2+/amplified expressing HER2 = HER2 IHC 2+, or IHC3+, or amplified low HER2 = HER2 IHC 2+/ not amplified *Currently enrolling | Data presented are interim data with a data cut-off date of August 1, 2021 9
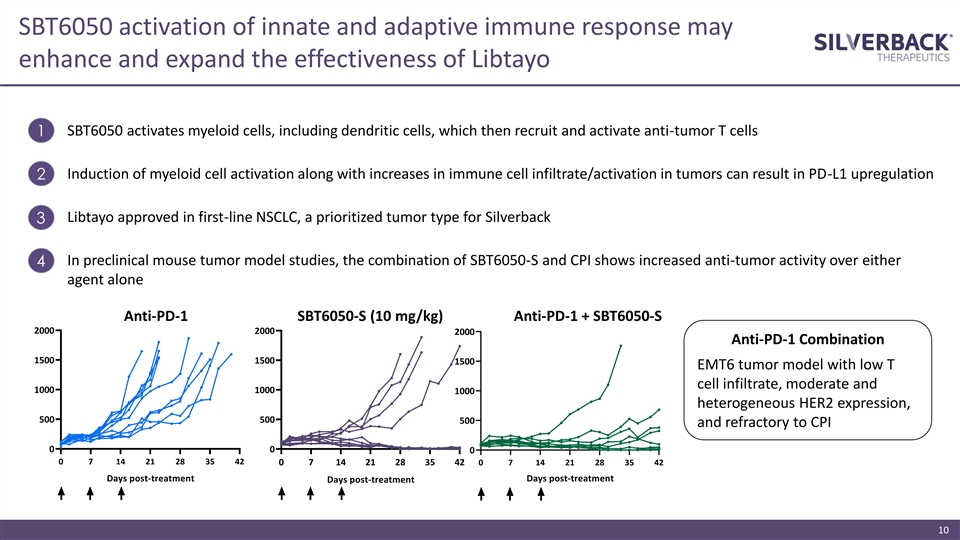
SBT6050 activation of innate and adaptive immune response may enhance and expand the effectiveness of Libtayo 1 SBT6050 activates myeloid cells, including dendritic cells, which then recruit and activate anti-tumor T cells Induction of myeloid cell activation along with increases in immune cell infiltrate/activation in tumors can result in PD-L1 upregulation 2 Libtayo approved in first-line NSCLC, a prioritized tumor type for Silverback 3 In preclinical mouse tumor model studies, the combination of SBT6050-S and CPI shows increased anti-tumor activity over either 4 agent alone Anti-PD-1 SBT6050-S (10 mg/kg) Anti-PD-1 + SBT6050-S 2000 2000 2000 Anti-PD-1 Combination 1500 1500 1500 EMT6 tumor model with low T cell infiltrate, moderate and 1000 1000 1000 heterogeneous HER2 expression, 500 500 500 and refractory to CPI 0 0 0 0 7 14 21 28 35 42 0 7 14 21 28 35 42 0 7 14 21 28 35 42 Days post-treatment Days post-treatment Days post-treatment 10SBT6050 activation of innate and adaptive immune response may enhance and expand the effectiveness of Libtayo 1 SBT6050 activates myeloid cells, including dendritic cells, which then recruit and activate anti-tumor T cells Induction of myeloid cell activation along with increases in immune cell infiltrate/activation in tumors can result in PD-L1 upregulation 2 Libtayo approved in first-line NSCLC, a prioritized tumor type for Silverback 3 In preclinical mouse tumor model studies, the combination of SBT6050-S and CPI shows increased anti-tumor activity over either 4 agent alone Anti-PD-1 SBT6050-S (10 mg/kg) Anti-PD-1 + SBT6050-S 2000 2000 2000 Anti-PD-1 Combination 1500 1500 1500 EMT6 tumor model with low T cell infiltrate, moderate and 1000 1000 1000 heterogeneous HER2 expression, 500 500 500 and refractory to CPI 0 0 0 0 7 14 21 28 35 42 0 7 14 21 28 35 42 0 7 14 21 28 35 42 Days post-treatment Days post-treatment Days post-treatment 10

Combination with Enhertu and with Tukysa + Herceptin +/- capecitabine are supported by a strong scientific and clinical rationale Enhertu | Herceptin+Tukysa +/- capecitabine Combination with SBT6050 Drive immunogenic tumor cell death and » Activates DCs, potentially enhancing presentation of neoantigens and T 1 release of tumor neoantigens cell activation Comprised of trastuzumab, capable of ADCC » Induces cytokines that amplify ADCC by NK cells 2 and ADCP » Downmodulates SIRPα on myeloid cells, increasing ADCP through attenuation of CD47-SIRPα interaction » Pertuzumab backbone is designed to combine with trastuzumab-based regimens Approved for 2L therapy in tumor types of » Designed to overcome common resistance mechanisms to 1L PD-(L)1 3 interest refractory patients » Addition of IO could deepen or prolong responses 11

Clinical development plans beyond monotherapy Combination regimen Strategic Initiative (estimated start) 3L+ mBC 2L+ NSCLC Combine with foundational IO therapy to lay Libtayo 3L+ GEA Accelerated approval in late line settings 3L+ GEA groundwork in early lines of treatment (4Q21) 2L+ NSCLC Enhertu 2L+ NSCLC Novel combination with HER2-based cytotoxic (1Q22) 2L+ GEA ADC to seek breakthroughs in 2L+ settings 1 Herceptin + Tukysa 2L+ mBC Novel combination with HER2-targeted therapies (1Q22) 2L+ CRC and chemo to seek breakthroughs in 2L+ settings 1. +/- capecitabine 12Clinical development plans beyond monotherapy Combination regimen Strategic Initiative (estimated start) 3L+ mBC 2L+ NSCLC Combine with foundational IO therapy to lay Libtayo 3L+ GEA Accelerated approval in late line settings 3L+ GEA groundwork in early lines of treatment (4Q21) 2L+ NSCLC Enhertu 2L+ NSCLC Novel combination with HER2-based cytotoxic (1Q22) 2L+ GEA ADC to seek breakthroughs in 2L+ settings 1 Herceptin + Tukysa 2L+ mBC Novel combination with HER2-targeted therapies (1Q22) 2L+ CRC and chemo to seek breakthroughs in 2L+ settings 1. +/- capecitabine 12

SBT6050 is designed to be used in combo with SOC agents such as CPIs and/or trastuzumab-based agents, potentially unlocking large market opportunities Estimated U.S. Incidence of Early-Line Estimated U.S. Incidence of Relapsed or HER2-Expressing Patients Refractory HER2-Expressing Patients 90,000 12,000 60,000 6,000 30,000 0 0 1 GEA Colorectal Bladder Uterine Pancreas H&N Ovarian Biliary Breast NSCLC Estimated HER2 Expression 30% 16-32% 23% 6-13% 9% 17-33% 7-33% 3-50% 5-19% 26% (IHC 2+/3+) & Amplifications FDA Approved HER2 ✓✓ Pathway Inhibitors FDA Approved HER2 ✓ Phase 2✓ Phase 2 Antibody Drug Conjugates FDA Approved Checkpoint Phase 3✓✓✓✓✓✓✓ Inhibitor Estimated early-line U.S. cases per year > 160k | Estimated relapsed or refractory U.S. cases per year > 48k 1. Gastroesophageal adenocarcinoma. Includes esophageal, gastric, gastroesophageal junction cancers 13SBT6050 is designed to be used in combo with SOC agents such as CPIs and/or trastuzumab-based agents, potentially unlocking large market opportunities Estimated U.S. Incidence of Early-Line Estimated U.S. Incidence of Relapsed or HER2-Expressing Patients Refractory HER2-Expressing Patients 90,000 12,000 60,000 6,000 30,000 0 0 1 GEA Colorectal Bladder Uterine Pancreas H&N Ovarian Biliary Breast NSCLC Estimated HER2 Expression 30% 16-32% 23% 6-13% 9% 17-33% 7-33% 3-50% 5-19% 26% (IHC 2+/3+) & Amplifications FDA Approved HER2 ✓✓ Pathway Inhibitors FDA Approved HER2 ✓ Phase 2✓ Phase 2 Antibody Drug Conjugates FDA Approved Checkpoint Phase 3✓✓✓✓✓✓✓ Inhibitor Estimated early-line U.S. cases per year > 160k | Estimated relapsed or refractory U.S. cases per year > 48k 1. Gastroesophageal adenocarcinoma. Includes esophageal, gastric, gastroesophageal junction cancers 13

SBT6050 administered alone or in combination with pembrolizumab has a manageable safety profile Most frequent* treatment-related treatment emergent adverse events (TEAEs), by maximum severity Part 1: SBT6050 Monotherapy (n=32) Part 3: SBT6050 + Pembrolizumab (n=8) Grade 1 Grade 2 Grade 3 Grade 1 Grade 2 Grade 3 Injection site reaction** 15 (46.9%) 11 (34.4%) 1 (3.1%) 5 (62.5%) 2 (25%) 0 Pyrexia 11 (34.4%) 9 (28.1%) 3 (9.4%) 3 (37.5%) 4 (50%) 0 Chills 14 (43.8%) 9 (28.1%) 0 3 (37.5%) 2 (25%) 0 Hypotension 5 (15.6%) 4 (12.5%) 6 (18.8%) 2 (25%) 4 (50%) 0 Nausea 6 (18.8%) 8 (25%) 1 (3.1%) 1 (12%) 4 (50%) 0 Vomiting 5 (15.6%) 9 (28.1%) 0 3 (37.5%) 0 0 Fatigue 0 7 (21.9%) 0 1 (12.5%) 1 (12.5%) 0 * ≥ 20% patients overall in Parts 1 and 3 ** Includes Injection Site Rash • No ≥ Grade 4 treatment-related TEAEs reported • No treatment-related TEAEs led to discontinuation • Grade 3 DLTs observed in Part 1 only and resolved with supportive care. These included hypotension, hypoxia, ISR and fever • 7 of the 8 patients who reported DLTs continued treatment at a reduced dose • Transient decreases in hemoglobin are similar across all dose levels 14SBT6050 administered alone or in combination with pembrolizumab has a manageable safety profile Most frequent* treatment-related treatment emergent adverse events (TEAEs), by maximum severity Part 1: SBT6050 Monotherapy (n=32) Part 3: SBT6050 + Pembrolizumab (n=8) Grade 1 Grade 2 Grade 3 Grade 1 Grade 2 Grade 3 Injection site reaction** 15 (46.9%) 11 (34.4%) 1 (3.1%) 5 (62.5%) 2 (25%) 0 Pyrexia 11 (34.4%) 9 (28.1%) 3 (9.4%) 3 (37.5%) 4 (50%) 0 Chills 14 (43.8%) 9 (28.1%) 0 3 (37.5%) 2 (25%) 0 Hypotension 5 (15.6%) 4 (12.5%) 6 (18.8%) 2 (25%) 4 (50%) 0 Nausea 6 (18.8%) 8 (25%) 1 (3.1%) 1 (12%) 4 (50%) 0 Vomiting 5 (15.6%) 9 (28.1%) 0 3 (37.5%) 0 0 Fatigue 0 7 (21.9%) 0 1 (12.5%) 1 (12.5%) 0 * ≥ 20% patients overall in Parts 1 and 3 ** Includes Injection Site Rash • No ≥ Grade 4 treatment-related TEAEs reported • No treatment-related TEAEs led to discontinuation • Grade 3 DLTs observed in Part 1 only and resolved with supportive care. These included hypotension, hypoxia, ISR and fever • 7 of the 8 patients who reported DLTs continued treatment at a reduced dose • Transient decreases in hemoglobin are similar across all dose levels 14
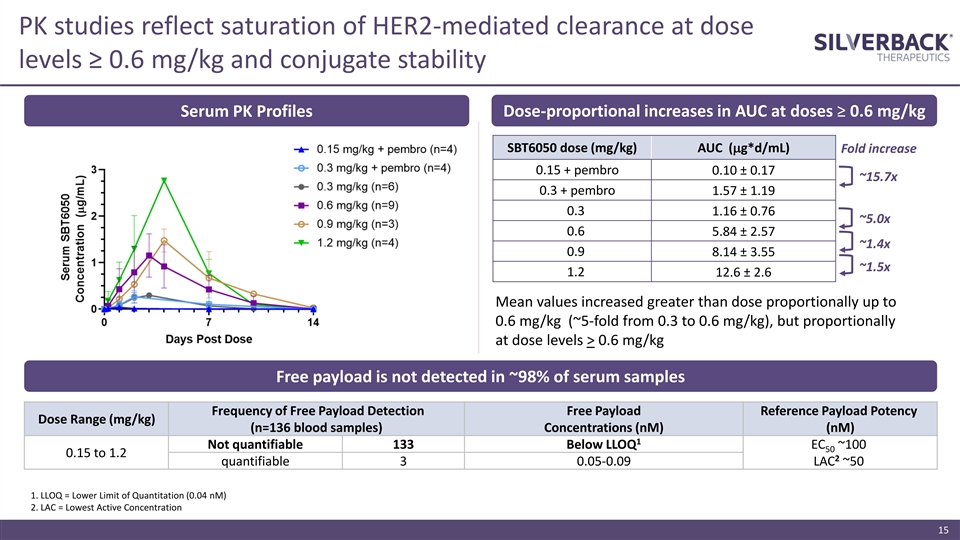
PK studies reflect saturation of HER2-mediated clearance at dose levels ≥ 0.6 mg/kg and conjugate stability Serum PK Profiles Dose-proportional increases in AUC at doses ≥ 0.6 mg/kg SBT6050 dose (mg/kg) AUC (mg*d/mL) Fold increase 0.15 + pembro 0.10 ± 0.17 ~15.7x 0.3 + pembro 1.57 ± 1.19 0.3 1.16 ± 0.76 ~5.0x 0.6 5.84 ± 2.57 ~1.4x 0.9 8.14 ± 3.55 ~1.5x 1.2 12.6 ± 2.6 Mean values increased greater than dose proportionally up to 0.6 mg/kg (~5-fold from 0.3 to 0.6 mg/kg), but proportionally at dose levels > 0.6 mg/kg Free payload is not detected in ~98% of serum samples Frequency of Free Payload Detection Free Payload Reference Payload Potency Dose Range (mg/kg) (n=136 blood samples) Concentrations (nM) (nM) 1 Not quantifiable 133 Below LLOQ EC ~100 50 0.15 to 1.2 2 quantifiable 3 0.05-0.09 LAC ~50 1. LLOQ = Lower Limit of Quantitation (0.04 nM) 2. LAC = Lowest Active Concentration 15PK studies reflect saturation of HER2-mediated clearance at dose levels ≥ 0.6 mg/kg and conjugate stability Serum PK Profiles Dose-proportional increases in AUC at doses ≥ 0.6 mg/kg SBT6050 dose (mg/kg) AUC (mg*d/mL) Fold increase 0.15 + pembro 0.10 ± 0.17 ~15.7x 0.3 + pembro 1.57 ± 1.19 0.3 1.16 ± 0.76 ~5.0x 0.6 5.84 ± 2.57 ~1.4x 0.9 8.14 ± 3.55 ~1.5x 1.2 12.6 ± 2.6 Mean values increased greater than dose proportionally up to 0.6 mg/kg (~5-fold from 0.3 to 0.6 mg/kg), but proportionally at dose levels > 0.6 mg/kg Free payload is not detected in ~98% of serum samples Frequency of Free Payload Detection Free Payload Reference Payload Potency Dose Range (mg/kg) (n=136 blood samples) Concentrations (nM) (nM) 1 Not quantifiable 133 Below LLOQ EC ~100 50 0.15 to 1.2 2 quantifiable 3 0.05-0.09 LAC ~50 1. LLOQ = Lower Limit of Quantitation (0.04 nM) 2. LAC = Lowest Active Concentration 15

Induction of PD biomarkers of myeloid cell activation observed across all dose levels and generally plateau at 0.6 mg/kg IP-10 MCP-1 IL-6 5000 3000 30000 20000 4000 2000 10000 3000 1000 1000 2000 75 1000 50 25 0 0 0 Part 1: SBT6050 Monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 0.6 mg/kg 1.2 mg/kg 0.30 mg/kg + 400 mg pembro For MCP-1 and IP-10, peak levels were significantly higher (unpaired t-test, p ≤0.05) at 0.6 mg/kg vs. lower dose levels, while no significant differences in peak levels were observed across the 0.6 to 1.2 mg/kg dose levels for any analyte 16 IP-10 (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak MCP-1 (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak IL-6 (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline PeakInduction of PD biomarkers of myeloid cell activation observed across all dose levels and generally plateau at 0.6 mg/kg IP-10 MCP-1 IL-6 5000 3000 30000 20000 4000 2000 10000 3000 1000 1000 2000 75 1000 50 25 0 0 0 Part 1: SBT6050 Monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 0.6 mg/kg 1.2 mg/kg 0.30 mg/kg + 400 mg pembro For MCP-1 and IP-10, peak levels were significantly higher (unpaired t-test, p ≤0.05) at 0.6 mg/kg vs. lower dose levels, while no significant differences in peak levels were observed across the 0.6 to 1.2 mg/kg dose levels for any analyte 16 IP-10 (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak MCP-1 (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak IL-6 (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak

Induction of IFNg, a biomarker of T and NK cell activation, observed across all dose levels and generally plateaus at 0.6 mg/kg Activation of DCs in lymph nodes drives expansion of IFNg polyfunctional tumor reactive T cells 1500 Lymph Node Tumor 1000 500 Dendritic cell 200 150 100 Antigen (from tumor) 50 0 Naïve T cell Activated tumor-specific T cell Part 1: SBT6050 Monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 0.6 mg/kg 1.2 mg/kg 0.30 mg/kg + 400 mg pembro 17 IFNγ (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline PeakInduction of IFNg, a biomarker of T and NK cell activation, observed across all dose levels and generally plateaus at 0.6 mg/kg Activation of DCs in lymph nodes drives expansion of IFNg polyfunctional tumor reactive T cells 1500 Lymph Node Tumor 1000 500 Dendritic cell 200 150 100 Antigen (from tumor) 50 0 Naïve T cell Activated tumor-specific T cell Part 1: SBT6050 Monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 0.6 mg/kg 1.2 mg/kg 0.30 mg/kg + 400 mg pembro 17 IFNγ (pg/mL) Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak Baseline Peak

PD activity is maintained with repeat dosing IP-10 MCP-1 IL-6 6000 3000 8000 2000 6000 4000 4000 1000 2000 2000 75 50 1000 25 0 0 0 IFNg 600 Part 1: SBT6050 Monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 400 0.6 mg/kg 1.2 mg/kg 0.30 mg/kg + 400 mg pembro 200 0 18 IP-10 (pg/mL) IFNg (pg/mL) Dose 1 Dose 1 Dose 4 Dose 4 Dose 1 Dose 1 Dose 4 Dose 4 Dose 1 Dose 1 Dose 4 Dose 4 Dose 1 Dose 1 Dose 4 Dose 4 Dose 1 Dose 1 Dose 4 Dose 4 Dose 1 Dose 1 Dose 4 Dose 4 MCP-1 (pg/mL) Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 IL-6 (pg/mL) Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4 Dose 1 Dose 4

SBT6050 payload is detected on tumor cells and in intratumoral macrophages, supporting the proposed mechanism of action in the TME SBT6050 payload is detected on tumor cells and in intratumoral macrophages of patients dosed at 0.6 mg/kg HER2 IHC 1+ breast cancer HER2 IHC 3+ breast cancer 19SBT6050 payload is detected on tumor cells and in intratumoral macrophages, supporting the proposed mechanism of action in the TME SBT6050 payload is detected on tumor cells and in intratumoral macrophages of patients dosed at 0.6 mg/kg HER2 IHC 1+ breast cancer HER2 IHC 3+ breast cancer 19

SBT6050 demonstrated early signals of anti-tumor activity in tumor types prioritized for expansion cohorts Part 1: SBT6050 monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 0.6 mg/kg 1.2 mg/kg 0.3 mg/kg + 400 mg pembro Figure includes patients with tumor types prioritized for expansion cohorts (breast, gastroesophageal, NSCLC), who have restaging CT scans evaluable per RECIST 20SBT6050 demonstrated early signals of anti-tumor activity in tumor types prioritized for expansion cohorts Part 1: SBT6050 monotherapy Part 3: SBT6050 + pembrolizumab 0.3 mg/kg 0.9 mg/kg 0.15 mg/kg + 400 mg pembro 0.6 mg/kg 1.2 mg/kg 0.3 mg/kg + 400 mg pembro Figure includes patients with tumor types prioritized for expansion cohorts (breast, gastroesophageal, NSCLC), who have restaging CT scans evaluable per RECIST 20

Adverse events do not change with repeat dosing; PR maintained while off study Partial Response 1 Stable Disease Progressive Disease Non-Evaluable Time Off-Study Part 1: SBT6050 monotherapy 0.3 mg/kg 0.9 mg/kg 0.6 mg/kg 1.2 mg/kg Part 3: SBT6050 combination with pembrolizumab 0.15 mg/kg + 400 mg pembro 0.30 mg/kg + 400 mg pembro • Overall response in patients with RECIST-evaluable CT scans (n=24) was PR: n=1, SD: n=8, PD: n=15. Figure includes patients with tumor types prioritized for expansion cohorts (breast, gastroesophageal, NSCLC), who have restaging CT scans evaluable per RECIST • Interim data as of August 1, 2021 1. Patient classified as progressive disease based on a new 5mm CNS lesion, but remains on study and demonstrated a 3% reduction in target lesions 21Adverse events do not change with repeat dosing; PR maintained while off study Partial Response 1 Stable Disease Progressive Disease Non-Evaluable Time Off-Study Part 1: SBT6050 monotherapy 0.3 mg/kg 0.9 mg/kg 0.6 mg/kg 1.2 mg/kg Part 3: SBT6050 combination with pembrolizumab 0.15 mg/kg + 400 mg pembro 0.30 mg/kg + 400 mg pembro • Overall response in patients with RECIST-evaluable CT scans (n=24) was PR: n=1, SD: n=8, PD: n=15. Figure includes patients with tumor types prioritized for expansion cohorts (breast, gastroesophageal, NSCLC), who have restaging CT scans evaluable per RECIST • Interim data as of August 1, 2021 1. Patient classified as progressive disease based on a new 5mm CNS lesion, but remains on study and demonstrated a 3% reduction in target lesions 21

SBT6050 conferred clinical benefit to patients with heavily pre-treated, advanced solid tumors NSCLC Breast Cancer Bladder Cancer Breast Cancer Breast Cancer Gastric Cancer HER2 IHC 2+ HER2 IHC 3+ HER2 IHC 2+ HER2 IHC 3+ HER2 IHC 3+ HER2 IHC 3+ Not amplified Amplification unknown 67F 73F 60M 48F 40F 49M Age 0.3 mg/kg 0.3 mg/kg 0.6 mg/kg 1.2 mg/kg 0.3 mg/kg 0.3 mg/kg Dose monotherapy monotherapy monotherapy monotherapy plus pembro plus pembro (decreased to 0.6 mg/kg at dose 3) 26 weeks 33 weeks >8 weeks and >21 weeks and >8 weeks and >8 weeks and Treatment (11 doses) (17 doses) remains on remains on remains on remains on Duration treatment treatment, per treatment treatment investigator decision 3 prior lines with 7+ prior lines 2 prior lines 4 prior lines 3+ prior lines 1 prior line including Prior Lines progression on prior including HER2-ADC including anti-PD-L1 including HER2-ADC, including HER2- HER2 targeted of Therapy PD-1 treatment and HER2 targeted and cisplatin- anti-PD-L1, and based cytotoxic ADC therapy therapy gemcitabine HER2 targeted and HER2 targeted therapy therapy Confirmed Stable Disease Stable Disease Progressive Disease Stable Disease Stable Disease Best Partial Response (+2%) (-2.7%) (-3% in target (-20%) (0%) Response (-55%) Maintained stable lesions) Decreasing tumor Response ongoing at 36 disease through 24- PD based on new marker (CA19-9 weeks from first dose week scan 5mm CNS lesion decrease from 135 to 64 U/mL) 22SBT6050 conferred clinical benefit to patients with heavily pre-treated, advanced solid tumors NSCLC Breast Cancer Bladder Cancer Breast Cancer Breast Cancer Gastric Cancer HER2 IHC 2+ HER2 IHC 3+ HER2 IHC 2+ HER2 IHC 3+ HER2 IHC 3+ HER2 IHC 3+ Not amplified Amplification unknown 67F 73F 60M 48F 40F 49M Age 0.3 mg/kg 0.3 mg/kg 0.6 mg/kg 1.2 mg/kg 0.3 mg/kg 0.3 mg/kg Dose monotherapy monotherapy monotherapy monotherapy plus pembro plus pembro (decreased to 0.6 mg/kg at dose 3) 26 weeks 33 weeks >8 weeks and >21 weeks and >8 weeks and >8 weeks and Treatment (11 doses) (17 doses) remains on remains on remains on remains on Duration treatment treatment, per treatment treatment investigator decision 3 prior lines with 7+ prior lines 2 prior lines 4 prior lines 3+ prior lines 1 prior line including Prior Lines progression on prior including HER2-ADC including anti-PD-L1 including HER2-ADC, including HER2- HER2 targeted of Therapy PD-1 treatment and HER2 targeted and cisplatin- anti-PD-L1, and based cytotoxic ADC therapy therapy gemcitabine HER2 targeted and HER2 targeted therapy therapy Confirmed Stable Disease Stable Disease Progressive Disease Stable Disease Stable Disease Best Partial Response (+2%) (-2.7%) (-3% in target (-20%) (0%) Response (-55%) Maintained stable lesions) Decreasing tumor Response ongoing at 36 disease through 24- PD based on new marker (CA19-9 weeks from first dose week scan 5mm CNS lesion decrease from 135 to 64 U/mL) 22
Safety profile, PK, and PD data support a projected RP2D of 0.6 mg/kg At the 0.6 mg/kg dose level: ✓ Safety and tolerability profile consistent with an immune activator and manageable ✓ Serum PK suggests HER2 target saturation ✓ Pharmacodynamic markers indicative of myeloid, T/NK cell activation reach a plateau ✓ Payload is detected in intratumoral macrophages and on tumor cells ✓ Signals of anti-tumor activity, as single agent or in combo, observed at doses at or above 0.15 mg/kg 23Safety profile, PK, and PD data support a projected RP2D of 0.6 mg/kg At the 0.6 mg/kg dose level: ✓ Safety and tolerability profile consistent with an immune activator and manageable ✓ Serum PK suggests HER2 target saturation ✓ Pharmacodynamic markers indicative of myeloid, T/NK cell activation reach a plateau ✓ Payload is detected in intratumoral macrophages and on tumor cells ✓ Signals of anti-tumor activity, as single agent or in combo, observed at doses at or above 0.15 mg/kg 23

SBT6290 comprises the same TLR8 agonist linker-payload used in SBT6050, SBT6290 conjugated to a proprietary Nectin4-directed monoclonal antibody ▪ Nectin4 is a clinically validated target by Seagen through the 2019 accelerated approval of ADC enfortumab vedotin (Padcev) in bladder cancer ▪ SBT6290 is tuned for activity in settings of Nectin4 moderate to high expression ▪ Preclinical studies demonstrate a similar functional profile to SBT6050, with robust anti-tumor activity and upregulation of key cytokines and chemokines in tumor that are indicative of myeloid and T/NK cell activation ▪ Non-GLP toxicology studies with SC administration in NHP indicate a favorable Tumor-targeting antigen: Nectin4 therapeutic window Target cell: myeloid cells ▪ Pre-IND alignment with FDA on preclinical, CMC, and clinical plan was achieved in February 2021 Payload: proprietary TLR8 agonist ▪ GLP toxicology study completed, with IND filing on track for the fourth quarter of 2021 Next milestones: • 4Q 2021 - submit IND • 1Q 2022 - initiate Phase 1 dose- escalation 24SBT6290 comprises the same TLR8 agonist linker-payload used in SBT6050, SBT6290 conjugated to a proprietary Nectin4-directed monoclonal antibody ▪ Nectin4 is a clinically validated target by Seagen through the 2019 accelerated approval of ADC enfortumab vedotin (Padcev) in bladder cancer ▪ SBT6290 is tuned for activity in settings of Nectin4 moderate to high expression ▪ Preclinical studies demonstrate a similar functional profile to SBT6050, with robust anti-tumor activity and upregulation of key cytokines and chemokines in tumor that are indicative of myeloid and T/NK cell activation ▪ Non-GLP toxicology studies with SC administration in NHP indicate a favorable Tumor-targeting antigen: Nectin4 therapeutic window Target cell: myeloid cells ▪ Pre-IND alignment with FDA on preclinical, CMC, and clinical plan was achieved in February 2021 Payload: proprietary TLR8 agonist ▪ GLP toxicology study completed, with IND filing on track for the fourth quarter of 2021 Next milestones: • 4Q 2021 - submit IND • 1Q 2022 - initiate Phase 1 dose- escalation 24

SBT6290 is selective for Nectin4 and blocks TIGIT:Nectin4 interaction SBT6290 is Selective for Nectin4 SBT6290 binding domain blocked TIGIT binding to Nectin4-expressing tumor cells Nectin Family Members Binding Affinity Nectin4 <1 pM 100 Nectin1 No binding detected; affinity is 75 Nectin2 >1µM Nectin3 50 SBT6290 Binds With High Affinity to Tumor Cells Expressing 25 Nectin4 0 SBT6290 mAb Isotype control Medium 25 % Inhibition of TIGIT Binding

SBT6290 activates human myeloid cells in a Nectin4- and Fc-dependent manner SBT6290 Activity is Nectin4-Dependent SBT6290 Activity Requires Fc Engagement pos neg Nectin4 cell line Nectin4 cell line pos Nectin4 cell line 26SBT6290 activates human myeloid cells in a Nectin4- and Fc-dependent manner SBT6290 Activity is Nectin4-Dependent SBT6290 Activity Requires Fc Engagement pos neg Nectin4 cell line Nectin4 cell line pos Nectin4 cell line 26
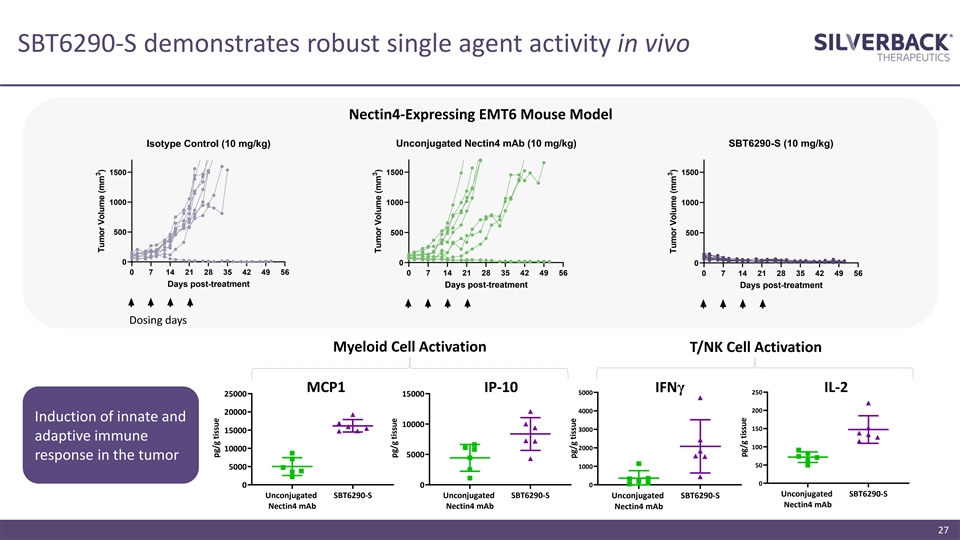
SBT6290-S demonstrates robust single agent activity in vivo Nectin4-Expressing EMT6 Mouse Model Isotype Control (10 mg/kg) Unconjugated Nectin4 mAb (10 mg/kg) SBT6290-S (10 mg/kg) 1500 1500 1500 1000 1000 1000 500 500 500 0 0 0 0 7 14 21 28 35 42 49 56 0 7 14 21 28 35 42 49 56 0 7 14 21 28 35 42 49 56 Days post-treatment Days post-treatment Days post-treatment Dosing days Myeloid Cell Activation T/NK Cell Activation MCP1 IP-10 IFNγ IL-2 5000 250 25000 15000 4000 200 20000 Induction of innate and 10000 150 3000 15000 adaptive immune 100 2000 10000 5000 response in the tumor 50 1000 5000 0 0 0 0 Unconjugated SBT6290-S Unconjugated SBT6290-S Unconjugated SBT6290-S Unconjugated SBT6290-S Nectin4 mAb Nectin4 mAb Nectin4 mAb Nectin4 mAb 27 3 Tumor Volume (mm ) pg/g tissue 3 Tumor Volume (mm ) pg/g tissue pg/g tissue 3 Tumor Volume (mm ) pg/g tissueSBT6290-S demonstrates robust single agent activity in vivo Nectin4-Expressing EMT6 Mouse Model Isotype Control (10 mg/kg) Unconjugated Nectin4 mAb (10 mg/kg) SBT6290-S (10 mg/kg) 1500 1500 1500 1000 1000 1000 500 500 500 0 0 0 0 7 14 21 28 35 42 49 56 0 7 14 21 28 35 42 49 56 0 7 14 21 28 35 42 49 56 Days post-treatment Days post-treatment Days post-treatment Dosing days Myeloid Cell Activation T/NK Cell Activation MCP1 IP-10 IFNγ IL-2 5000 250 25000 15000 4000 200 20000 Induction of innate and 10000 150 3000 15000 adaptive immune 100 2000 10000 5000 response in the tumor 50 1000 5000 0 0 0 0 Unconjugated SBT6290-S Unconjugated SBT6290-S Unconjugated SBT6290-S Unconjugated SBT6290-S Nectin4 mAb Nectin4 mAb Nectin4 mAb Nectin4 mAb 27 3 Tumor Volume (mm ) pg/g tissue 3 Tumor Volume (mm ) pg/g tissue pg/g tissue 3 Tumor Volume (mm ) pg/g tissue

Nectin4 is overexpressed in bladder, TNBC, H&N, and NSCLC, among other indications, unlocking a large opportunity in an untapped market Nectin4 Overexpression Across Select Tumor Types 101,000 58,000 48,000 21,000 10,000 11,000 3,000 2,000 181k estimated early-line U.S. cases per year Bladder TNBC H&N NSCLC Estimated Nectin4 1 1 1 2 73k estimated relapsed or Moderate – High 60-83% 53-78% 18-59% 30-58% IHC Expression refractory U.S. cases per year Estimated U.S. Incidence of Early-Line Estimated U.S. Incidence of Relapsed or Nectin4-Expressing Patients Refractory Nectin4-Expressing Patients Nectin4-Targeted Therapies in Development Bladder Breast Lung H&N GEC 3 Approved Ph 3 Ph 2 – Solid Tumor Basket Study Ph 1 – Solid Tumor Basket Study 1 2 3 Challita-Eid et al Cancer Research 2016, et al. | Takano et al Cancer Research 2009 | Padcev accelerated approval 28Nectin4 is overexpressed in bladder, TNBC, H&N, and NSCLC, among other indications, unlocking a large opportunity in an untapped market Nectin4 Overexpression Across Select Tumor Types 101,000 58,000 48,000 21,000 10,000 11,000 3,000 2,000 181k estimated early-line U.S. cases per year Bladder TNBC H&N NSCLC Estimated Nectin4 1 1 1 2 73k estimated relapsed or Moderate – High 60-83% 53-78% 18-59% 30-58% IHC Expression refractory U.S. cases per year Estimated U.S. Incidence of Early-Line Estimated U.S. Incidence of Relapsed or Nectin4-Expressing Patients Refractory Nectin4-Expressing Patients Nectin4-Targeted Therapies in Development Bladder Breast Lung H&N GEC 3 Approved Ph 3 Ph 2 – Solid Tumor Basket Study Ph 1 – Solid Tumor Basket Study 1 2 3 Challita-Eid et al Cancer Research 2016, et al. | Takano et al Cancer Research 2009 | Padcev accelerated approval 28
SBT8230 provides opportunity to further realize potential of SBT8230 TLR8 agonism with liver-localized activity, if approved ▪ Potent IFNγ-mediated immune response and seroconversion, which TLR8 agonism has been shown to drive, is key determinant of achieving a functional cure in cHBV ▪ Clinical validation provided by Gilead’s untargeted, orally administered TLR8 agonist small molecule selgantolimod (GS-9688) Liver-targeting antigen: ASGR1 ▪ SBT8230 binds to ASGR1 (GalNAc target) and is combinable with RNAi Target cell: myeloid cells approaches and other cHBV therapies Payload: proprietary TLR8 agonist ▪ Designed to achieve exposure not possible with untargeted, systemically administered TLR8 agonists Indication: cHBV ▪ Exploratory NHP toxicology study demonstrates wide therapeutic Next milestone: window • 1Q 2022 - initiate IND-enabling tox studies ▪ Early CMC activities initiated, including selection of the clone and creation of a master cell bank 29

ASGR1-TLR8 potently activated human myeloid cells, resulting in a robust IFNg response TNFa: Myeloid Activation, Potent IFNγ Activation Increased Viral Ag Presentation 90000 15000 10000 Lead conjugate Unconjugated mAb 60000 5000 Control conjugate 0 0.01 0.1 1 10 100 1000 30000 Concentration (nM) IL-18: Synergized with IL-12: DC Activation IL-12 for Th1 Response 0 100 0.01 0.1 1 10 100 1000 30000 80 Concentration (nM) 20000 60 40 10000 Lead conjugate 20 Unconjugated mAb 0 0 0.01 0.1 1 10 100 1000 0.01 0.1 1 10 100 1000 Control conjugate Concentration (nM) Concentration (nM) 30 IL-12 (pg/mL) TNFa (pg/mL) IL-18 (pg/mL) IFNg (pg/mL)ASGR1-TLR8 potently activated human myeloid cells, resulting in a robust IFNg response TNFa: Myeloid Activation, Potent IFNγ Activation Increased Viral Ag Presentation 90000 15000 10000 Lead conjugate Unconjugated mAb 60000 5000 Control conjugate 0 0.01 0.1 1 10 100 1000 30000 Concentration (nM) IL-18: Synergized with IL-12: DC Activation IL-12 for Th1 Response 0 100 0.01 0.1 1 10 100 1000 30000 80 Concentration (nM) 20000 60 40 10000 Lead conjugate 20 Unconjugated mAb 0 0 0.01 0.1 1 10 100 1000 0.01 0.1 1 10 100 1000 Control conjugate Concentration (nM) Concentration (nM) 30 IL-12 (pg/mL) TNFa (pg/mL) IL-18 (pg/mL) IFNg (pg/mL)

ASGR1-S reduces Hepatitis B surface antigen (HBsAg) and drives seroconversion in AAV-HBV mouse model HBsAg plasma levels Seroconversion p= < 0.0001 p= 0.02 ASGR1-S lowered average plasma viral DNA titers 2.5 logs 31ASGR1-S reduces Hepatitis B surface antigen (HBsAg) and drives seroconversion in AAV-HBV mouse model HBsAg plasma levels Seroconversion p= < 0.0001 p= 0.02 ASGR1-S lowered average plasma viral DNA titers 2.5 logs 31

Multiple preclinical programs to expand ImmunoTAC platform IO TLR8 Programs ▪ Two additional undisclosed IO targets may enable us to expand coverage of solid tumor indications ▪ Same TLR8 linker-payload utilized in SBT6050 and SBT6290 and similar in vitro functional profile Liver-Directed TGFβRi ImmunoTAC for Liver Fibrosis ▪ Designed for liver-localized TGFβ signaling inhibition for anti-fibrotic effects ▪ Designed to inhibit the TGFβR directly for complete pathway inhibition ▪ Blockade of TGFβ/SMAD signaling in hepatocytes in mice (CCl4 model) prevents liver fibrosis Additional Discovery Programs ▪ Additional ImmunoTAC conjugates comprised of novel payload classes in preclinical development and entering in vivo models 32Multiple preclinical programs to expand ImmunoTAC platform IO TLR8 Programs ▪ Two additional undisclosed IO targets may enable us to expand coverage of solid tumor indications ▪ Same TLR8 linker-payload utilized in SBT6050 and SBT6290 and similar in vitro functional profile Liver-Directed TGFβRi ImmunoTAC for Liver Fibrosis ▪ Designed for liver-localized TGFβ signaling inhibition for anti-fibrotic effects ▪ Designed to inhibit the TGFβR directly for complete pathway inhibition ▪ Blockade of TGFβ/SMAD signaling in hepatocytes in mice (CCl4 model) prevents liver fibrosis Additional Discovery Programs ▪ Additional ImmunoTAC conjugates comprised of novel payload classes in preclinical development and entering in vivo models 32

Led by a veteran team with a track record of advancing transformative therapies Leadership Team Board of Directors Peter Thompson, MD Co-Founder, Chairman Vickie Capps Rob Hershberg, MD, PhD Laura Shawver, PhD Valerie Odegard, PhD Naomi Hunder, MD Jonathan Piazza Chief Executive Officer President, CSO Chief Medical Officer Chief Financial Officer Saqib Islam, JD Maria Koehler, MD, PhD Andrew Powell, JD Jonathan Root, MD Thilo Schroeder, MD Sateesh Natarajan, PhD Jeffrey Pepe, JD, PhD Scott Moorefield, PhD Russ Hawkinson Laura Shawver, PhD SVP, CMC SVP, General Counsel SVP, Business Development SVP, Finance 33Led by a veteran team with a track record of advancing transformative therapies Leadership Team Board of Directors Peter Thompson, MD Co-Founder, Chairman Vickie Capps Rob Hershberg, MD, PhD Laura Shawver, PhD Valerie Odegard, PhD Naomi Hunder, MD Jonathan Piazza Chief Executive Officer President, CSO Chief Medical Officer Chief Financial Officer Saqib Islam, JD Maria Koehler, MD, PhD Andrew Powell, JD Jonathan Root, MD Thilo Schroeder, MD Sateesh Natarajan, PhD Jeffrey Pepe, JD, PhD Scott Moorefield, PhD Russ Hawkinson Laura Shawver, PhD SVP, CMC SVP, General Counsel SVP, Business Development SVP, Finance 33

Corporate highlights ImmunoTAC conjugates are designed to unlock a new class of targeted immuno-oncology agents that direct a 1 myeloid cell agonist to the tumor microenvironment for localized activation Emerging clinical data supports proof-of-mechanism for localized TLR8 agonism and the ImmunoTAC platform, 2 evidenced by the robust activation of innate and adaptive immune response seen in patients SBT6050 has demonstrated early signals of anti-tumor activity as a monotherapy and in combination with a 3 PD-1 inhibitor, with a manageable safety profile consistent with an active IO agent Clinical development plan to evaluate SBT6050 in combinations designed to have long-term benefit in early lines 4 of treatment, including combo with anti-PD1, with Enhertu and with Herceptin/Tukysa Positive readthrough to Silverback’s TLR8 pipeline with value-generating milestones expected in the next 6-18 5 months, including anticipated initiation of SBT6290 (Nectin4) Ph1 study and SBT8230 (HBV) Ph1-enabling studies 34Corporate highlights ImmunoTAC conjugates are designed to unlock a new class of targeted immuno-oncology agents that direct a 1 myeloid cell agonist to the tumor microenvironment for localized activation Emerging clinical data supports proof-of-mechanism for localized TLR8 agonism and the ImmunoTAC platform, 2 evidenced by the robust activation of innate and adaptive immune response seen in patients SBT6050 has demonstrated early signals of anti-tumor activity as a monotherapy and in combination with a 3 PD-1 inhibitor, with a manageable safety profile consistent with an active IO agent Clinical development plan to evaluate SBT6050 in combinations designed to have long-term benefit in early lines 4 of treatment, including combo with anti-PD1, with Enhertu and with Herceptin/Tukysa Positive readthrough to Silverback’s TLR8 pipeline with value-generating milestones expected in the next 6-18 5 months, including anticipated initiation of SBT6290 (Nectin4) Ph1 study and SBT8230 (HBV) Ph1-enabling studies 34

Thank youThank you
Serious News for Serious Traders! Try StreetInsider.com Premium Free!
You May Also Be Interested In
- Breaking New Ground: Cleanfarms Champions Circular Economy for Canadian Agricultural Plastics
- StrikePoint Provides Corporate Update
- The 25th Jeonju International Film Festival Kicks off on May 1st in Jeonju, Korea
Create E-mail Alert Related Categories
SEC FilingsSign up for StreetInsider Free!
Receive full access to all new and archived articles, unlimited portfolio tracking, e-mail alerts, custom newswires and RSS feeds - and more!
