

Form 10-K ENSIGN GROUP, INC For: Dec 31
 Tweet
Tweet Share
ShareUNITED STATES
SECURITIES AND EXCHANGE COMMISSION
Washington, D.C. 20549
_____________________________
FORM 10-K
| ANNUAL REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934. | |||||
For the fiscal year ended December 31 , 2022
OR
| TRANSITION REPORT PURSUANT TO SECTION 13 OR 15(d) OF THE SECURITIES EXCHANGE ACT OF 1934. | |||||
For the transition period from to . | |||||
Commission file number: 001-33757
_____________________________

THE ENSIGN GROUP, INC .
(Exact Name of Registrant as Specified in Its Charter)
| (State or Other Jurisdiction of | (I.R.S. Employer | ||||
| Incorporation or Organization) | Identification No.) | ||||
(Address of Principal Executive Offices and Zip Code)
(949 ) 487-9500
(Registrant’s Telephone Number, Including Area Code)
_____________________________
Securities registered pursuant to Section 12(b) of the Act:
| Title of each class | Trading Symbol(s) | Name of each exchange on which registered | ||||||
Securities registered pursuant to Section 12(g) of the Act:
None
| Indicate by check mark: | |||||||||||||||||||||||||||||||||||||||||
| if the registrant is a well-known seasoned issuer, as defined in Rule 405 of the Securities Act. | þ | ☐ | No | ||||||||||||||||||||||||||||||||||||||
| if the registrant is not required to file reports pursuant to Section 13 or Section 15(d) of the Act. | ☐ | Yes | þ | ||||||||||||||||||||||||||||||||||||||
| whether the registrant (1) has filed all reports required to be filed by Section 13 or 15(d) of the Securities Exchange Act of 1934 during the preceding 12 months (or for such shorter period that the registrant was required to file such reports), and (2) has been subject to such filing requirements for the past 90 days. | þ | ☐ | No | ||||||||||||||||||||||||||||||||||||||
| whether the registrant has submitted electronically, every Interactive Data File required to be submitted pursuant to Rule 405 of Regulation S-T (§232.405 of this chapter) during the preceding 12 months (or for such shorter period that the registrant was required to submit such files). | þ | ☐ | No | ||||||||||||||||||||||||||||||||||||||
| whether the registrant is a large accelerated filer, an accelerated filer, non-accelerated filer, a smaller reporting company, or an emerging growth company. See the definitions of “large accelerated filer,” “accelerated filer,” “smaller reporting company,” and "emerging growth company" in Rule 12b-2 of the Exchange Act: | |||||||||||||||||||||||||||||||||||||||||
| þ | Accelerated filer | ☐ | Non-accelerated filer | ☐ | Smaller reporting company | Emerging growth company | |||||||||||||||||||||||||||||||||||
| If an emerging growth company, indicate if the registrant has elected not to use the extended transition period for complying with any new or revised financial accounting standards provided pursuant to Section 13(a) of the Exchange Act. | ☐ | Yes | ☐ | No | |||||||||||||||||||||||||||||||||||||
| whether the registrant has filed a report on and attestation to its management's assessment of the effectiveness of its internal control over financial reporting under Section-404(b) of the Sarbanes-Oxley Act (15 U.S.C. 7262(b)) by the registered public accounting firm that prepared or issued its audit report. | Yes | ☐ | No | ||||||||||||||||||||||||||||||||||||||
| If securities are registered pursuant to Section 12(b) of the Act, whether the financial statements of the registrant included in the filing reflect the correction of an error to previously issued financial statements. | ☐ | Yes | þ | No | |||||||||||||||||||||||||||||||||||||
| whether any of those error corrections are restatements that required a recovery analysis of incentive-based compensation received by any of the registrant’s executive officers during the relevant recovery period pursuant to §240.10D-1(b). | ☐ | Yes | þ | No | |||||||||||||||||||||||||||||||||||||
| whether the registrant is a shell company (as defined in Rule 12b-2 of the Exchange Act). | ☐ | Yes | No | ||||||||||||||||||||||||||||||||||||||
| As of June 30, 2022, the aggregate market value of the Registrant's Common Stock held by non-affiliates was: | |||||||||||||||||||||||||||||||||||||||||
| Common Stock | $ | ||||||||||||||||||||||||||||||||||||||||
The aggregate market value of Common Stock was computed by reference to the closing price as of the last business day of the registrant's most recently completed second fiscal quarter. Shares of Common Stock held by each executive officer, director and each person owning more than 10% of the outstanding Common Stock of the registrant have been excluded (in the amount of $1,511,035,000) in that such persons may be deemed to be affiliates of the registrant. This determination of affiliate status is not necessarily a conclusive determination for other purposes. | |||||||||||||||||||||||||||||||||||||||||
As of January 30, 2023, 55,732,114 shares of the registrant’s common stock, $0.001 par value, were outstanding.
THE ENSIGN GROUP, INC.
INDEX TO ANNUAL REPORT ON FORM 10-K
FOR THE FISCAL YEAR ENDED DECEMBER 31, 2022
TABLE OF CONTENTS
| PART I | |||||||||||
| PART II. | |||||||||||
| PART III. | |||||||||||
| PART IV. | |||||||||||
CAUTIONARY NOTE REGARDING FORWARD-LOOKING STATEMENTS
This Annual Report on Form 10-K contains forward-looking statements, which include, but are not limited to our expected future financial position, results of operations, cash flows, financing plans, business strategy, budgets, capital expenditures, competitive positions, growth opportunities and plans and objectives of management. Forward-looking statements can often be identified by words such as “anticipates,” “expects,” “intends,” “plans,” “predicts,” “believes,” “seeks,” “estimates,” “may,” “will,” “should,” “would,” “could,” “potential,” “continue,” “ongoing,” similar expressions, and variations or negatives of these words. These statements are subject to the safe harbors under Private Securities Litigation Reform Act of 1995. These statements are not guarantees of future performance and are subject to risks, uncertainties and assumptions that are difficult to predict. Additionally, many of these risks and uncertainties are currently, and in the future may continue to be, amplified by the impacts of the coronavirus (COVID-19) pandemic, including the response efforts of federal, state and local government authorities, businesses, individuals and us. Therefore, our actual results could differ materially and adversely from those expressed in any forward-looking statements as a result of various factors, some of which are listed under the section “Risk Factors” in Part I, Item 1A of this Annual Report on Form 10-K. Accordingly, you should not rely upon forward-looking statements as predictions of future events. These forward-looking statements speak only as of the date of this Annual Report, and are based on our current expectations, estimates and projections about our industry and business, management's beliefs, and certain assumptions made by us, all of which are subject to change. We undertake no obligation to revise or update publicly any forward-looking statement for any reason, except as otherwise required by law.
As used in this Annual Report on Form 10-K, the words, "Ensign," "Company," “we,” “our” and “us” refer to The Ensign Group, Inc. and its consolidated subsidiaries. All of our operating subsidiaries, the Service Center (defined below) and our wholly-owned captive insurance subsidiary (the Captive Insurance) and captive real estate investment trust called Standard Bearer Healthcare REIT, Inc. (Standard Bearer) are operated by separate, wholly-owned, independent subsidiaries that have their own management, employees and assets. References herein to the consolidated “Company” and “its” assets and activities, as well as the use of the terms “we,” “us,” “our” and similar terms in this Annual Report on Form 10-K is not meant to imply, nor should it be construed as meaning, that The Ensign Group, Inc. has direct operating assets, employees or revenue, or that any of the subsidiaries are operated by The Ensign Group.
The Ensign Group, Inc. is a holding company with no direct operating assets, employees or revenues. In addition, certain of our wholly-owned independent subsidiaries, collectively referred to as the Service Center, provide centralized accounting, payroll, human resources, information technology, legal, risk management and other centralized services to the other operating subsidiaries through contractual relationships with such subsidiaries. The Captive Insurance provides some claims-made coverage to our operating subsidiaries for general and professional liability, as well as for certain workers' compensation insurance liabilities. Standard Bearer owns and manages our real estate business.
The Service Center address is 29222 Rancho Viejo Rd Suite 127, San Juan Capistrano, CA 92675, and our telephone number is (949) 487-9500. Our corporate website is located at www.ensigngroup.net. The information contained in, or that can be accessed through, our website does not constitute a part of this Annual Report on Form 10-K.
EnsignTM is our United States trademark. All other trademarks and trade names appearing in this annual report are the property of their respective owners.
PART I.
ITEM 1. BUSINESS
Founded in 1999, The Ensign Group, Inc. ("Ensign") is a holding company with subsidiaries that provide skilled nursing, senior living and rehabilitative services, as well as other ancillary businesses (including mobile diagnostics and medical transportation), in 13 states. As part of our investment strategy, we also acquire, lease and own healthcare real estate to service the post-acute care continuum through acquisition and investment opportunities in healthcare properties. For the year ended December 31, 2022, we generated approximately 96.1% of our revenue from our skilled nursing facilities. The remainder of our revenue is primarily generated from our real estate properties, senior living services and other ancillary services.
OPERATIONS
Overview
As of December 31, 2022, we offered skilled nursing, senior living and rehabilitative care services through 271 skilled nursing and senior living facilities. Of the 271 facilities, we operated 192 facilities under long-term lease arrangements and have options to purchase 11 of those 192 facilities. Our real estate portfolio includes 108 owned real estate properties, which included 79 facilities operated and managed by us, 29 senior living operations leased to and operated by The Pennant Group, Inc., or Pennant, as part of the spin-off transaction that occurred in October 2019, and the Service Center location. Of the 29 real estate operations leased to Pennant, one senior living operation is located on the same real estate property as a skilled nursing facility that we own and operate.
Our Unique Approach and Structure
The name "Ensign" is synonymous with a "flag" or a "standard" and refers to our goal of setting the standard by which all others in our industry are measured. We believe that through our efforts and leadership, we can foster a new level of patient care and professional competence at our affiliated operating subsidiaries, and set a new industry standard for each patient we service. We view healthcare services primarily as a local business. We believe our success is largely driven by our proven ability to build strong relationships with key stakeholders in local healthcare communities, in part, by leveraging our reputation for providing superior care. Accordingly, our brand strategy and organizational structure promotes the empowerment of local leadership and staff to make their facility the “operation of choice” in their community. This is accomplished by allowing local leadership to discern and address the unique needs and priorities of healthcare professionals, customers and other stakeholders in the local community or market, and then work to create a superior service offering for, and reputation in, their particular community. This local empowerment is unique within the healthcare services industry.
We believe that our localized approach encourages prospective patients and referral sources to choose or recommend our local operations. In addition, our leaders are enabled and motivated to share real-time operating data and otherwise benchmark clinical and operational performance against their peers in order to improve clinical care, enhance patient satisfaction and augment operational efficiencies, promoting the sharing of best practices.
We organize our operating subsidiaries into portfolio companies, which we believe has enabled us to maintain a local, field-driven organizational structure, attract additional qualified leadership talent, and to identify, acquire, and improve operations at a generally faster rate. Each of our portfolio companies has its own leader. These leaders, who are generally taken from the ranks of operational CEOs, serve as leadership resources within their own portfolio companies, and have the primary responsibility for recruiting qualified talent, finding potential acquisition targets, and identifying other internal and external growth opportunities. We believe this organizational structure has improved the quality of our recruiting and will continue to facilitate successful acquisitions.
Since we spun-off our owned real estate properties into a public real estate investment trust (REIT) in 2014, we have continued to expand our real estate portfolio. Following the real estate spin-off, we have acquired and currently own 108 real estate properties, including 29 real estate properties that are leased to a third party under triple-net long-term leases. We manage and operate the remaining real estate properties, including the Service Center location. We are committed to growing our real estate portfolio, which we believe will further enhance our earnings and maximize long-term shareholder value.
1
To continue with our growth strategy on our real estate portfolio, in January 2022, we formed Standard Bearer. Standard Bearer owns and manages our real estate business. We believe the REIT structure allows us to better demonstrate the growing value of our owned real estate and provide us with an efficient vehicle for future acquisitions of properties that could be operated by Ensign affiliates or other third parties. We believe this structure gives us new pathways to growth with transactions we would not have considered in the past. Standard Bearer intends to qualify and elect to be taxed as a REIT, for U.S. federal income tax purposes, commencing with its taxable year ended December 31, 2022. The real estate portfolio in Standard Bearer consists of 103 of our 108 owned real estate properties. For further details on the Standard Bearer REIT, refer to Note 7, Standard Bearer, in Notes to the Consolidated Financial Statements of this Annual Report on Form 10-K.
SEGMENTS
We have two reportable segments: (1) skilled services, which includes the operation of skilled nursing facilities and rehabilitation therapy services and (2) Standard Bearer, which is comprised of select properties owned by us through our captive REIT and leased to skilled nursing and senior living operations, including our own operating subsidiaries and third party operators.
We also report an “all other” category that includes operating results from our senior living operations, mobile diagnostics, transportation, other real estate and other ancillary operations. These businesses are neither significant individually, nor in aggregate and therefore do not constitute a reportable segment. Our Chief Executive Officer, who is our chief operating decision maker, or CODM, reviews financial information at the operating segment level. We have presented our segment results in this Annual Report on Form 10-K on a comparative basis to conform to the segment structure. For more information about our operating segments, as well as financial information, see Part II Item 7. Management’s Discussion and Analysis of Financial Condition and Results of Operations and Note 8, Business Segments of the Notes to the Consolidated Financial Statements.
Skilled Services
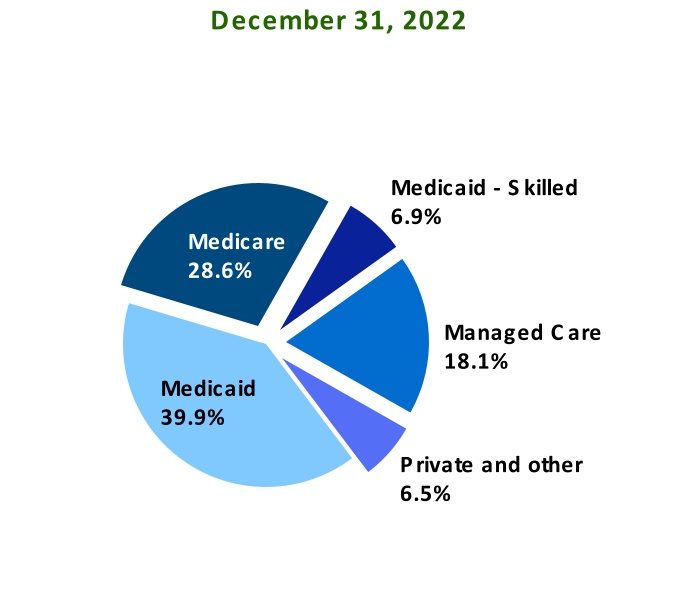
As of December 31, 2022, our skilled nursing companies provided skilled nursing care at 260 operations, with 28,130 operational beds, in Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin. We provide short and long-term nursing care services for patients with chronic conditions, prolonged illness, and the elderly. Our residents are often high-acuity patients that come to our facilities to recover from strokes, cardiovascular and respiratory conditions, neurological conditions, joint replacements, and other muscular or skeletal disorders. We use interdisciplinary teams of experienced medical professionals to provide services prescribed by physicians. These medical professionals provide individualized comprehensive nursing care to our short-stay and long-stay patients. Many of our skilled nursing facilities are equipped to provide specialty care, such as on-site dialysis, ventilator care, cardiac and pulmonary management. We also provide standard services such as room and board, special nutritional programs, social services, recreational activities, entertainment, and other services. We are dedicated to ensuring our residents are happy, comfortable, and motivated to achieve their health goals through the provision of quality care. We generate our skilled services revenue from Medicaid, Medicare, managed care, commercial insurance, and private pay. During the year ended December 31, 2022, approximately 46.8% and 28.6% of our skilled services revenue was derived from Medicaid and Medicare programs, respectively.
Standard Bearer
We engage in the acquisition and leasing of skilled nursing and senior living properties. We generate rental revenue primarily by leasing post-acute care properties we acquired to healthcare operators under triple-net lease arrangements, whereby the tenant is solely responsible for the costs related to the property, including property taxes, insurance and maintenance and repair costs, subject to certain exceptions. As of December 31, 2022, our real estate portfolio within Standard Bearer is comprised of 103 real estate properties located in Arizona, California, Colorado, Idaho, Kansas, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin. Of these properties, 75 are leased to affiliated skilled nursing facilities wholly-owned and managed by us and 29 are leased to senior living operations wholly-owned and managed by Pennant. Of the 29 real estate operations leased to Pennant, one senior living operation is located on the same real estate property as a skilled nursing facility that we own and operate. During the year ended December 31, 2022, we generated rental revenues of $72.9 million, of which $58.0 million was derived from affiliated wholly-owned healthcare operators, and therefore eliminated in consolidation.
2
Other
Revenue from our senior living operations, other real estate, mobile diagnostics and other ancillary operations comprise approximately 4.1% of our annual revenue.
Senior Living — As of December 31, 2022, we had an aggregate of 3,021 senior living units across 37 operations, of which 26 are located on the same site location as our skilled nursing care operations. Our senior living communities located in Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Texas, Utah and Washington, provide residential accommodations, activities, meals, housekeeping and assistance in the activities of daily living to seniors who are independent or who require some support, but not the level of nursing care provided in a skilled nursing operation. Our independent living units are non-licensed independent living apartments in which residents are independent and require no support with the activities of daily living.
Our senior living operations comprise approximately 2.2% of our annual revenue. We generate revenue at these units primarily from private pay sources, with a small portion derived from Medicaid or other state-specific programs. Specifically, during the year ended December 31, 2022, approximately 63.1% of our senior living revenue was derived from private pay sources.
Ancillary — As of December 31, 2022, we held a majority membership interest of ancillary operations located in Arizona, California, Colorado, Idaho, Texas, Utah and Washington. We have invested in and are exploring new business lines that are complementary to our existing skilled services and senior living services. These new business lines consist of mobile ancillary services, including digital x-ray, ultrasound, electrocardiograms, sub-acute services, dialysis, respiratory and patient transportation to people in their homes or at long-term care facilities. To date these businesses were not meaningful contributors to our operating results.
GROWTH
We have an established track record of successful acquisitions. Much of our historical growth can be attributed to implementing our expertise in acquiring real estate or leasing both under-performing and performing post-acute care operations and transforming them into market leaders in clinical quality, staff competency, employee loyalty and financial performance. With each acquisition, we apply our core operating expertise to improve these operations, both clinically and financially. In years where pricing has been high, we have focused on the integration and improvement of our existing operating subsidiaries while limiting our acquisitions to strategically situated properties.
From January 1, 2012 through December 31, 2022, we acquired 223 facilities, which added 18,443 operational skilled nursing beds and 5,000 senior living units to our operating subsidiaries, which included the operations that were contributed to Pennant. The following table summarizes cumulative skilled nursing and senior living operation, operational skilled nursing bed and senior living unit counts at the end of 2012 and each of the last five years to reflect our growth over a ten-year period and five-year period as a result of the acquisition of these facilities:
| December 31, | ||||||||||||||||||||||||||||||||||||||
2012(2) | 2018(2) | 2019(1)(2) | 2020 | 2021 | 2022 | |||||||||||||||||||||||||||||||||
| Cumulative number of skilled nursing and senior living operations | 108 | 244 | 223 | 228 | 245 | 271 | ||||||||||||||||||||||||||||||||
| Cumulative number of operational skilled nursing beds | 10,215 | 19,615 | 22,625 | 23,172 | 25,032 | 28,130 | ||||||||||||||||||||||||||||||||
| Cumulative number of senior living units | 1,677 | 5,664 | 2,154 | 2,254 | 2,237 | 3,021 | ||||||||||||||||||||||||||||||||
(1) Number of operational beds and number of operations for 2018 and 2019 include operational beds and operations that we no longer operated. The number of operations and operational beds do not include the closed facilities beginning in the year of their closures.
(2) Included in the 2012 and 2018-2019 number of operational units and number of operations are the operational units and operations of senior living facilities that we transferred to Pennant in 2019. In 2019, the number of operations and operational units do not include operations transferred to Pennant.
We have also invested in new business lines that are complementary to our existing businesses, such as ancillary services. We plan to continue to grow our revenue and earnings by:
•continuing to grow our talent base and develop future leaders;
•increasing the overall percentage or “mix” of higher-acuity patients;
•focusing on organic growth and internal operating efficiencies;
•continuing to acquire additional operations in existing and new markets;
3
•expanding and renovating our existing operations, and
•strategically investing in and integrating other post-acute care healthcare businesses.
New Market CEO and New Ventures Programs. In order to broaden our reach into new markets, and in an effort to provide existing leaders in our company with the entrepreneurial opportunity and challenge of entering a new market and starting a new business, we established our New Market CEO program in 2006. Supported by our Service Center and other resources, a New Market CEO evaluates a target market, develops a comprehensive business plan, and relocates to the target market to find talent and connect with other providers, regulators and the healthcare community in that market, with the goal of ultimately acquiring businesses and establishing an operating platform for future growth. In addition, this program includes other lines of business that are closely related to the skilled nursing industry. The New Ventures program encourages our local leaders to evaluate service offerings with the goal of establishing an operating platform in new markets and new businesses. We believe that this program will not only continue to drive growth, but will also provide a valuable training ground for our next generation of leaders, who will have experienced the challenges of growing and operating a new business.
EXPANSIONS
During the year ended December 31, 2022, we expanded our operations and real estate portfolio through a combination of long-term leases and real estate purchases, with the addition of 23 stand-alone skilled nursing operations and one campus operation. Of these additions, Standard Bearer acquired the real estate of seven of the stand-alone skilled nursing operations, which were leased back to Ensign affiliated entities. In addition, we purchased the real estate of three skilled nursing properties which our affiliated operating subsidiaries already operated, further expanding our real estate portfolio. We also added five senior living operations that were transferred from Pennant, three of which are part of campuses operated by our affiliated operating subsidiaries. These new operations added a total of 3,058 operational skilled nursing beds and 674 operational senior living units to be operated by our affiliated operating subsidiaries. Additionally, we invested in new ancillary services that are complementary to our existing businesses.
Subsequent to December 31, 2022, we expanded our operations through long-term leases, with the addition of seventeen stand-alone skilled nursing operations. These new operations added 1,462 operational skilled nursing beds to be operated by our affiliated operating subsidiaries.
For further discussion of our acquisitions, see Note 9, Operation Expansions in the Notes to the Consolidated Financial Statements.
QUALITY OF CARE MEASURES
Improvement in Acquired Facilities. In December 2008, the Centers for Medicare and Medicaid Services (CMS) introduced the Five-Star Quality Rating System to help consumers, their families and caregivers compare nursing homes more easily. The Five-Star Quality Rating System gives each skilled nursing operation a rating between one and five stars in various categories. We have a strong history of quickly improving the quality of care in the facilities we acquire. Thus, as new assessments are conducted post-acquisition, the star ratings see consistent improvement. At the time of acquisition, the majority of our facilities have 1 and 2-Star ratings.
Over the last few years, CMS had modified the Star rating requirements. These changes have been significant and made it more difficult to achieve a 4 or 5-Star rating. The 2019 changes resulted in nursing centers losing stars in their "Quality" and "Staffing" ratings, which negatively impacted the "Overall" ratings. Nevertheless, we continue to demonstrate strong performance in the Five-Star Quality Rating System. We believe compliance and quality outcomes are precursors to outstanding financial performance. Thus, we strive to aggressively increase quality and compliance in every facility we acquire, and to adjust our overall policies to adapt to CMS’s changing criteria for the Five-Star Quality Rating System. As a result of the COVID-19 pandemic, CMS temporarily waived certain reporting timeframes and suspended certain inspections that impacted the underlying data used for calculating star-ratings. This resulted in CMS freezing affected quality measures by only using data collected for periods not impacted by the COVID-19 waivers. CMS continues to change the way the star-rating is calculated, both through ongoing regulation changes and CMS's enactment or expiration of waivers regarding reporting and calculation requirements for five-star ratings. Therefore, depending on the changes, we may experience periods of time where the number of facilities with 4 or 5-Star ratings decline. The star-rating calculations resumed on January 27, 2021.
4
The table below summarizes the number of our facilities with 4 and 5-Star ratings since 2018:
| As of December 31, | |||||||||||||||||||||||||||||
| 2018 | 2019 | 2020 | 2021 | 2022 | |||||||||||||||||||||||||
| 4 and 5-Star Quality Rated skilled nursing facilities | 91 | 102 | 116 | 114 | 113 | ||||||||||||||||||||||||
Above-Average Ratings. Additionally, despite the fact that Ensign’s acquisition of facilities with 1 or 2-Star ratings skews our company-wide ratings, our mean score on the Five-Star Quality Rating System is 64.8%, which exceeds the national average score of 58.0%.
INDUSTRY TRENDS
The post-acute care industry has evolved to meet the growing demand for post-acute and custodial healthcare services generated by an aging population, increasing life expectancies and the trend toward shifting patient care to lower cost settings. The industry has evolved in recent years, which we believe has led to a number of favorable improvements in the industry, as described below:
•Shift of Patient Care to Lower Cost Alternatives — The growth of the senior population in the U.S. continues to increase healthcare costs, often faster than the available funding from government-sponsored healthcare programs. In response, federal and state governments have adopted cost-containment measures that encourage the treatment of patients in more cost-effective settings such as skilled nursing facilities, for which the staffing requirements and associated costs are often significantly lower than acute care hospitals and other post-acute care settings. As a result, skilled nursing facilities are generally serving a larger population of higher-acuity patients than in the past.
•Significant Acquisition and Consolidation Opportunities — The skilled nursing industry is large and highly fragmented, characterized predominantly by numerous local and regional providers. Due to the increasing demands from hospitals and insurance carriers to implement sophisticated and expensive reporting systems, we believe this fragmentation provides us with significant acquisition and consolidation opportunities.
•Improving Supply and Demand Balance — The number of skilled nursing facilities has declined modestly over the past several years. We expect that the supply and demand balance in the skilled nursing industry will continue to improve due to the shift of patient care to lower cost settings, an aging population and increasing life expectancies.
•Increased Demand Driven by Aging Populations — As seniors account for an increasing percentage of the total U.S. population, we believe the demand for skilled nursing and senior living services will continue to increase. According to the census projection released by the U.S. Census Bureau in early 2020, between 2016 and 2030, the number of individuals over 65 years old is projected to be one of the fastest growing segments of the United States population, growing from 16% to 21%. The Bureau expects this segment to increase nearly 50% to 73 million, as compared to the total U.S. population which is projected to increase by 10% over that time period. Furthermore, the generation currently retiring has accumulated less savings than prior generations, creating demand for more affordable senior housing and skilled nursing services. As a high-quality provider in lower cost settings, we believe we are well-positioned to benefit from this trend.
•Transition to Value-Based Payment Models — In response to rising healthcare spending in the United States, commercial, government and other payors are generally shifting away from fee-for-service (FFS) payment models towards value-based models, including risk-based payment models that tie financial incentives to quality, efficiency and coordination of care. We believe that patient-centered outcomes driven reimbursement models will continue to grow in prominence. Many of our operations already receive value-based payments, and as valued-based payment systems continue to increase in prominence, it is our view that our strong clinical outcomes will be increasingly rewarded.
5
•Accountable Care Organizations and Reimbursement Reform — A significant goal of U.S. federal health care reform is to transform the delivery of health care by changing reimbursement to reflect and support the quality and safety of care that providers deliver, increase efficiency, and reduce growth in spending. Reimbursement models that provide financial incentives to encourage efficiency, affordability, and high-quality care have been developed and implemented by government and commercial third-party payers. The most prolific of these models, the Accountable Care Organization (ACO) model, incentivizes groups of providers to share in savings that are achieved through the coordination of care and chronic disease management of an assigned patient population. Reimbursement methodology reform includes Value-Based Purchasing (VBP), in which a portion of provider reimbursement is redistributed based on relative performance, or improvement on designated economic, clinical quality, and patient satisfaction metrics. In addition, the Centers for Medicare and Medicaid Services (CMS) has implemented Episode-based demonstration, voluntary and mandatory payment initiatives that bundle acute care and post-acute care reimbursement. These bundled payment models incentivize cross-continuum care coordination and include financial and performance accountability for episodes of care. These reimbursement methodologies and similar programs are likely to continue and expand, both in government and commercial health plans. Many of our operations already participate in ACOs. With our focus on quality care and strong clinical outcomes, Ensign is well-positioned to benefit from these outcome-based payment models.
We believe the post-acute industry has been and will continue to be impacted by several other trends. The use of long-term care (LTC) insurance is increasing among seniors as a means of planning for the costs of skilled nursing services. In addition, as a result of increased mobility in society, reduction of average family size, and the increased number of two-wage earner couples, more residents are looking for alternatives outside the family for their care.
Our business is affected by seasonal fluctuations in occupancy and acuity which are most prominent when comparing the summer and winter months of the calendar year (including volatility arising from COVID-19).
REVENUE SOURCES
We derive revenue primarily from the Medicaid and Medicare programs, managed care and commercial insurance payors, and private pay patients. The majority of our revenue is derived from skilled nursing, which is highly dependent upon the Medicaid and Medicare programs. Thus, any changes to payment models, reimbursements and budgets impact our revenue, some positively and some negatively. A detailed discussion of the regulatory framework impacting our business is found in the Government Regulation section below. See also, Item 1A., Risk Factors.
A brief overview of each of our revenue sources is as follows:
Medicaid — Medicaid is a program financed by state funds and matching federal funds administered by the states and their political subdivisions, and often go by state-specific names, such as Medi-Cal in California and the Arizona Healthcare Cost Containment System in Arizona. Medicaid programs generally provide health benefits for qualifying individuals, and may supplement Medicare benefits for the disabled and for persons aged 65 and older meeting financial eligibility requirements. Medicaid reimbursement formulas are established by each state with the approval of the federal government in accordance with federal guidelines. Seniors who enter skilled nursing facilities as private pay clients can become eligible for Medicaid once they have substantially depleted their assets. Medicaid is generally the largest source of funding for most skilled nursing facilities.
Medicaid reimbursement varies from state to state and is based upon a number of different systems, including cost-based, prospective payment; case mixed adjusted payments and negotiated rate systems. Rates are subject to a state’s annual budgetary requirements and funding, statutory and regulatory changes and interpretations and rulings by individual state agencies and State Plan Amendments approved by CMS.
Medicaid typically covers patients that require standard room and board services and provides reimbursement rates that are generally lower than rates earned from other sources. We monitor our payor mix to measure the level received from each payor across each of our business units. We intend to continue to focus on enhancing our care offerings to accommodate more high acuity patients.
6
Approximately 81.9% of our Medicaid revenue comes from Arizona, California, Colorado, Texas, and Utah. In California, the state enacted legislation expanding their Medicaid program, which in recent years has continued to see budget increases, but may see Medicaid spending decrease in the 2022-2023 period. It is projected that California General Fund spending on California Medicaid will be $35.5 billion for the 2022-2023 budget year, which is a decrease of approximately $900 million from its 2022-2023 budget estimate. California also estimates that the 2023-2024 budget year's Medicaid spending will decrease by $1.3 billion to $34.2 billion. Over the longer term, however, California expects its Medicaid spending to increase, reaching more than $38 billiion by the 2026-2027 budget year. Texas is one of the remaining states that has not expanded Medicaid under the Affordable Care Act. Texas lawmakers have, in the past, underfunded Medicaid, requiring an infusion of state and federal funds. Funding for the 2022-2023 Texas biennium includes $25.1 billion in general revenue funds, which is a decrease of $400 million in general funds from the 2020-2021 biennium amounts. In Arizona, the state enacted legislation expanding their Medicaid program in 2013 but has seen decreased Medicaid enrollments in recent years. Their 2021 budget for the state Medicaid program included $1.9 billion from the general fund and the 2022 budget increased to over $1.92 billion. In Utah, a public referendum to expand the state’s Medicaid program succeeded in 2018, and in 2020 the Utah legislature fully implemented this Medicaid program expansion. Utah’s fiscal year 2021 Medicaid spending was $3.9 billion, and the state’s budget for 2022 fiscal year Medicaid spending, which will continue into 2023, is expected to be similar.
Medicare — Medicare is a federal program that provides healthcare benefits to individuals who are 65 years of age or older or are disabled. To achieve and maintain Medicare certification, a skilled nursing facility must sign a Medicare provider agreement and meet the CMS “Conditions of Participation” on an ongoing basis, as determined in periodic facility inspections or “surveys” conducted primarily by the state licensing agency in the state where the facility is located. Medicare pays for inpatient skilled nursing facility services under the prospective payment system (PPS). Under PPS, facilities are paid a predetermined amount per patient, per day, for certain services. Medicare Part A skilled nursing facility coverage is limited to 100 days per episode of illness for those beneficiaries who require daily care following discharge from an acute care hospital.
For Medicare beneficiaries who qualify for the Medicare Part A coverage, rehabilitation services are included in the per diem payment. For beneficiaries who do not meet the coverage criteria for Part A services, rehabilitation services may qualify for the services to be provided under Medicare Part B.
Managed Care and Private Insurance — Managed care patients consist of individuals who are insured by certain third-party entities, or who are Medicare beneficiaries who have assigned their Medicare benefits to a senior managed care organization plan. Another type of insurance, long-term care insurance, is also becoming more available to consumers, but is not expected to contribute significantly to industry revenues in the near term.
Private and Other Payors — Private and other payors consist primarily of individuals, family members or other third parties who directly pay for the services we provide.
Rental Revenue — Real estate rental revenue is generated by leasing post-acute care properties that we acquired to healthcare operators under triple-net lease arrangements, whereby the tenant is solely responsible for the costs related to the property, including property taxes, insurance and maintenance and repair costs, subject to certain exceptions.
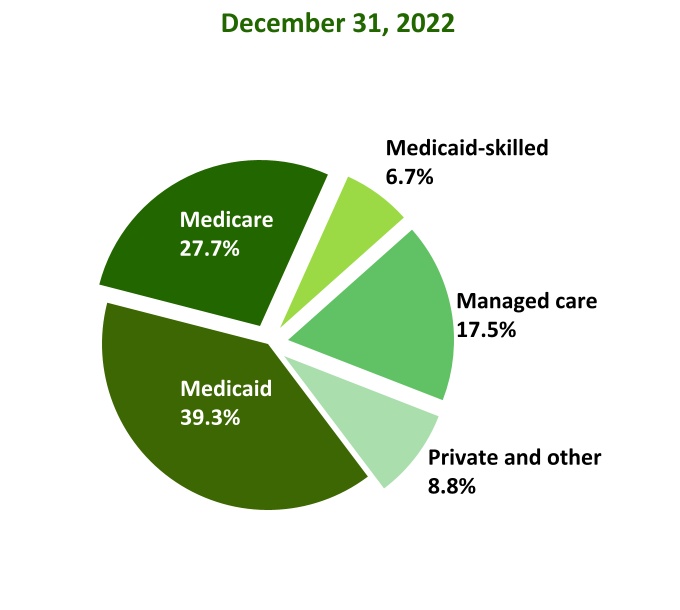
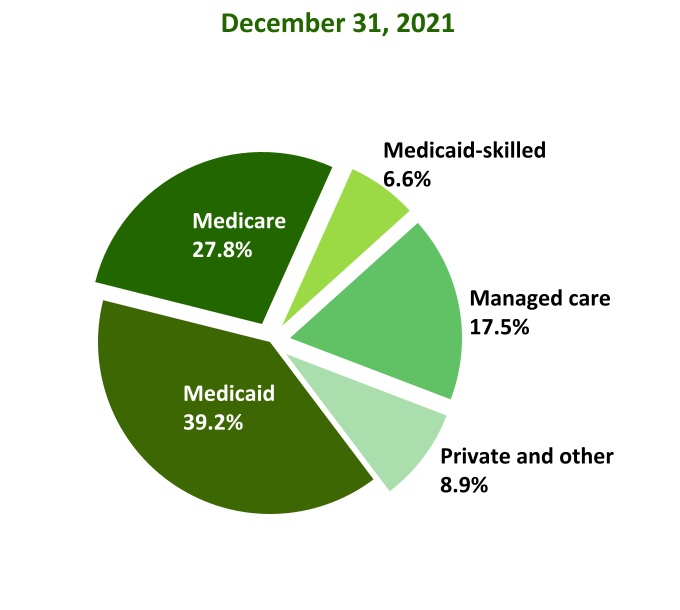
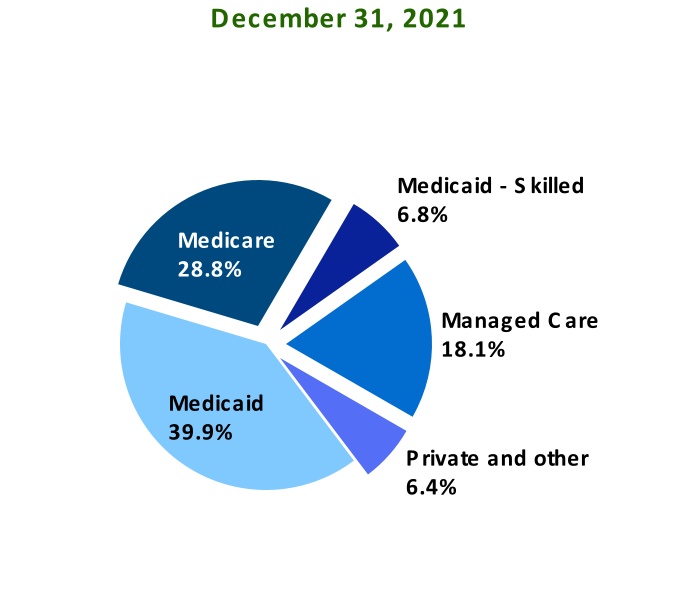
The following charts sets forth our total service revenue by payor source generated by our consolidated operations and skilled services segment as a percentage of total revenue for the years ended December 31, 2022 and 2021, respectively:
7
CONSOLIDATED SERVICE REVENUE BY PAYOR
SKILLED SERVICES REVENUE BY PAYOR
Payor Sources as a Percentage of Skilled Nursing Services — The following table sets forth our percentage of skilled nursing patient days by payor source:
| Year Ended December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Percentage of Skilled Nursing Days: | |||||||||||
| Medicare | 13.5 | % | 13.5 | % | |||||||
| Managed care | 13.1 | 13.0 | |||||||||
| Other skilled | 5.2 | 5.2 | |||||||||
| SKILLED MIX | 31.8 | 31.7 | |||||||||
| Private and other payors | 10.3 | 10.2 | |||||||||
| Medicaid | 57.9 | 58.1 | |||||||||
| TOTAL SKILLED NURSING | 100.0 | % | 100.0 | % | |||||||
8
REIMBURSEMENT FOR SPECIFIC SERVICES
Reimbursement for Skilled Nursing Services — Skilled nursing facility revenue is primarily derived from Medicaid, Medicare, managed care and private payors. Our skilled nursing operations provide Medicaid-covered services to eligible individuals consisting of nursing care, room and board and social services. In addition, states may, at their option, cover other services such as physical, occupational and speech therapies.
Historically, adjustments to reimbursement under Medicare and Medicaid have had a significant effect on our revenue and results of operations. Recently enacted, pending and proposed legislation and administrative rulemaking at the federal and state levels could have similar effects on our business. Efforts to impose reduced reimbursement rates, greater discounts and more stringent cost controls by government and other payors are expected to continue for the foreseeable future and could adversely affect our business, financial condition and results of operations. Additionally, any delay or default by the federal or state governments in making Medicare and/or Medicaid reimbursement payments could materially and adversely affect our business, financial condition and results of operations.
Reimbursement for Rehabilitation Therapy Services — Rehabilitation therapy revenue is primarily received from private pay, managed care and Medicare for services provided at skilled nursing operations and senior living operations. The payments are based on negotiated patient per diem rates or a negotiated fee schedule based on the type of service rendered.
Reimbursement for Senior Living — Senior living facility revenue is primarily derived from private pay patients at rates we established, with only a small portion of such revenue derived from state-specific programs such as Medicaid.
Reimbursement for Other Ancillary Services — Other ancillary revenue, such as mobile diagnostics and medical transportation, is primarily derived from Medicare Part B, Medicaid, managed care and private payors at rates we establish based upon the services we provide and market conditions in the area of operation.
RENTAL REVENUE
Rental revenue from third party rental property tenants — Standard Bearer's owned properties are leased pursuant to non-cancelable operating leases, generally with an initial term of 10 to 15 years. All of the post-acute care healthcare properties leased contain renewal options. The leases provide for fixed minimum base rent during the initial and renewal periods. Standard Bearer's leases contain provisions for specified annual increases over the rents of the prior year and those increases are generally computed on a calculation based on the Consumer Price Index.
Each lease is a triple net lease which requires the lessee to pay all taxes, insurance, maintenance and repairs, capital and non-capital expenditures and other costs necessary in the operations of the facilities. In addition, Standard Bearer's leases with third-parties are typically structured as master leases. The master leases consist of multiple leases, each with its own pool of properties, that have varying maturities and diversity in property geography.
If a lessee makes payments for taxes and insurance directly to a third-party on our behalf, we are required to exclude these payments from variable payments and from revenue recognition in our consolidated statements of income. Otherwise, tenant reimbursements paid to us for taxes and insurance are classified as additional rental revenue recognized by us on a gross basis.
Rental revenue from Ensign-affiliated tenants — Rental revenue from Ensign-affiliated operations is based on mutually agreed-upon base rents that are subject to change from time to time. Intercompany revenue is eliminated in consolidation, along with the corresponding intercompany rent expenses of the related healthcare facilities.
COMPETITION
The post-acute care industry is highly competitive, and we expect that the industry will become increasingly competitive in the future. The industry is highly fragmented and characterized by numerous local and regional providers, in addition to large national providers that have achieved geographic diversity and economies of scale. Our operating subsidiaries also compete with inpatient rehabilitation facilities and long-term acute care hospitals. Increasingly, we are competing with home health and community-based providers who have developed programs designed to provide services to seniors outside a facility-based setting, potentially decreasing the time they need the higher level of care provided in a skilled nursing facility. Competitiveness may vary significantly from location to location, depending upon factors such as the number of competing facilities, availability of services, expertise of staff, and the physical appearance and amenities of each location. We believe that the primary competitive factors in the post-acute care industry are:
9
•ability to attract and to retain qualified management and caregivers;
•reputation and achievements of quality healthcare outcomes;
•attractiveness and location of facilities;
•the expertise and commitment of the management team and employees; and
•community value, including amenities and ancillary services.
We seek to compete effectively in each market by establishing a reputation within the local community as the “operation of choice.” This means that the operation leaders are generally free to discern and address the unique needs and priorities of healthcare professionals, customers and other stakeholders in the local community or market, and then create a superior service offering and reputation for that particular community or market that is calculated to encourage prospective customers and referral sources to choose or recommend the operation.
Increased competition could limit our ability to attract and retain patients, maintain or increase rates or to expand our business. Some of our competitors have greater financial and other resources than we have, may have greater brand recognition and may be more established in their respective communities than we are. Competing companies may also offer newer facilities or different programs or services than we offer, and may therefore attract individuals who are currently patients of our facilities, potential patients of our facilities, or who are otherwise receiving our healthcare services. Other competitors may have lower expenses or other competitive advantages than us and, therefore, provide services at lower prices than we offer.
Our other services, such as senior living facilities and other ancillary services, also compete with local, regional, and national companies. The primary competitive factors in these businesses are similar to those for our skilled nursing facilities and include reputation, cost of services, quality of clinical services, responsiveness to patient/resident needs, location and the ability to provide support in other areas such as third-party reimbursement, information management and patient recordkeeping.
Our Standard Bearer segment competes for real property investments with healthcare providers, healthcare-related REITs, real estate partnerships, banks, private equity funds, venture capital funds and other investors. Some of these competitors are significantly larger and have greater financial resources and lower costs of capital than us. Our ability to compete successfully for real property investments will be determined by numerous factors, including our ability to identify suitable acquisition targets, our ability to negotiate acceptable terms for any such acquisition and our cost of capital in the event an acquisition requires debt or equity financing.
OUR COMPETITIVE STRENGTHS
We believe that we are well positioned to benefit from the ongoing changes within our industry. We believe that our ability to acquire, integrate and improve our facilities is a direct result of the following key competitive strengths:
Experienced and Dedicated Employees — We believe that our operating subsidiaries' employees are among the best in their respective industries. We believe each of our operating subsidiaries is led by an experienced and caring leadership team, including dedicated front-line care staff, who participates daily in the clinical and operational improvement of their individual operations. We have been successful in attracting, training, incentivizing and retaining a core group of outstanding business and clinical leaders to spearhead our operating subsidiaries. These leaders operate as separate local businesses. With broad local control, these talented leaders and their care staffs are able to quickly meet the needs of their patients and residents, employees and local communities, without waiting for permission to act or being bound to a “one-size-fits-all” corporate strategy.
Unique Incentive Programs — We believe that our employee compensation programs are unique within the industry. Employee stock options and performance bonuses, based on achieving target clinical quality, cultural, compliance and financial benchmarks, represent a significant component of total compensation for our operational leaders. We believe that these compensation programs assist us in encouraging our leaders and key employees to act with a shared ownership mentality. Furthermore, our leaders are motivated to help local operations within a defined “cluster” and "market," which is a group of geographically proximate operations that share clinical best practices, real-time financial data and other resources and information.
10
Staff and Leadership Development — We have a company-wide commitment to ongoing education, training and professional development. Accordingly, our operational leaders participate in regular training. Most participate in training sessions at Ensign University, our in-house educational system. Other training opportunities are generally offered via on-demand training tools, including podcasts. In addition, we offer weekly cultural and interactive educational topics including leadership development, our values, updates on Medicaid and Medicare billing requirements, updates on new regulations or legislation, infection control, COVID-19 clinical and regulations, emerging healthcare service alternatives and other relevant clinical, business and industry specific coursework. Additionally, we encourage and provide ongoing education classes for our clinical staff to maintain licensing and increase the breadth of their knowledge and expertise. We believe that our commitment to, and substantial investment in, ongoing education will further strengthen the quality of our operational leaders and staff, and the quality of the care they provide to our patients and residents.
Innovative Service Center Approach — We do not maintain a corporate headquarters; rather, we operate a Service Center to support the efforts of each operation. Our Service Center is a dedicated service organization that acts as a resource and provides centralized information technology, human resources, accounting, payroll, legal, risk management, educational and other back office support services, so that local leaders can focus on delivering top-quality care and efficient business operations. Our Service Center approach allows individual operations to function with the strength, synergies and economies of scale found in larger organizations, but without what we believe are the disadvantages of a top-down management structure or corporate hierarchy. We believe our Service Center approach is unique within the industry, and allows us to preserve the “one-operation-at-a-time” focus and culture that has contributed to our success.
Proven Track Record of Successful Acquisitions — We have established a disciplined acquisition strategy that is focused on selectively acquiring operations within our target markets. Our acquisition strategy is driven by our operations team. Prospective leaders are included in the decision-making process and compensated as these acquired operations reach pre-established clinical quality and financial benchmarks, helping to ensure that we only undertake acquisitions that key leaders believe can become clinically sound and contribute to our financial performance.
As of December 31, 2022, we have expanded to 271 facilities with an aggregate of 28,130 operational skilled nursing beds and 3,021 senior living units, through both long-term leases and purchases. We believe our experience in acquiring these operations and our demonstrated success in significantly improving their operations enables us to consider a broad range of acquisition targets. In addition, we believe we have developed expertise in transitioning newly acquired operations to our unique organizational culture and systems, which enables us to acquire operations with limited disruption to patients, residents and operating staff, while significantly improving quality of care. We have also constructed new facilities to target demand, which exists for high-end healthcare facilities when we determine that market conditions justify the cost of new construction in some of our markets.
Successful Real Estate Investment Strategy — As part of our Standard Bearer segment, we maintain a real estate portfolio of long-term healthcare facilities diversified by geographic location and operated by a diverse group of established healthcare providers. We are focused on selectively acquiring real estate properties based on our industry experience and opportunistic strategy, which we believe provides us with greater investment and purchasing opportunities. Due to our credit strength, we have the ability to acquire large portfolios of real estate properties; a portion of which can be managed and operated by our Ensign affiliated established healthcare leaders and a portion of which can be leased to third parties.
As of December 31, 2022, our real estate portfolio consists of 108 owned facilities, which include properties leased to and operated by third parties and properties we managed and operated. We believe our real estate investment strategy has allowed us to accumulate a portfolio that aids our healthcare operators in improving performance and generating additional returns through leases with third parties.
Reputation for Quality Care — We believe that we have achieved a reputation for high-quality and cost-effective care and services to our patients and residents within the communities we serve. We believe that our achievement of quality outcomes enhances our reputation for quality, that when coupled with the integrated services that we offer, allows us to attract patients that require more intensive and medically complex care and generally result in higher reimbursement rates than lower acuity patients.
11
Community Focused Approach — We view our services primarily as a local, community-based business. Our local leadership-centered management culture enables each operation's nursing support staff and leaders to meet the unique needs of their patients and local communities. We believe that our commitment to this “one-operation-at-a-time” philosophy helps to ensure that each operation, its patients, their family members and the community will receive the individualized attention they need. By serving our patients, their families, the community and our fellow healthcare professionals, we strive to make each individual business the operation of choice in its local community.
We further believe that when choosing a healthcare provider, consumers usually choose a person or people they know and trust, rather than a corporation or business. Therefore, rather than pursuing a traditional organization-wide branding strategy, we actively seek to develop the operations brand at the local level, serving and marketing one-on-one to caregivers, our patients, their families, the community and our fellow healthcare professionals in the local market.
Investment in Information Technology — We utilize information technology that enables our operational leaders to access, and to share with their peers, both clinical and financial performance data in real time. Armed with relevant and current information, our operation leaders and their management teams are able to share best practices and the latest information, adjust to challenges and opportunities on a timely basis, improve quality of care, mitigate risk and improve both clinical outcomes and financial performance. We have also invested in specialized healthcare technology systems to assist our nursing and support staff. We have installed software and touch-screen interface systems in each operation to enable our clinical staff to more efficiently monitor and deliver patient care and record patient information. We believe these systems have improved the quality of our medical and billing records, while improving the productivity of our staff.
OUR GROWTH STRATEGY
We believe that the following strategies are primarily responsible for our growth to date, and will continue to drive the growth of our business:
Grow Talent Base and Develop Future Leaders — Our primary growth strategy is to expand our talent base and develop future leaders. A key component of our organizational culture is our belief that strong local leadership is a primary key to the success of each operation. While we believe that significant acquisition opportunities exist, we have generally followed a disciplined approach to growth that permits us to acquire an operation only when we believe, among other things, that we will have qualified leadership for that operation. To develop these leaders, we have a rigorous “CEO-in-Training Program” that attracts proven business leaders from various industries and backgrounds, and provides them the knowledge and hands-on training they need to successfully lead one of our operating subsidiaries. We generally have between 25 and 30 prospective administrators progressing through the various stages of this training program, which is generally much more rigorous, hands-on and intensive than the minimum 1,000 hours of training mandated by the licensing requirements of most states where we do business. Once administrators are licensed and assigned to an operation, they continue to learn and develop in our operational Chief Executive Officer Program (CEO Program), which facilitates the continued development of these talented business leaders into outstanding operational chief executive officers, through regular peer review, our Ensign University and on-the-job training.
In addition, our Chief Operating Officer Program (COO Program) recruits and trains highly qualified Directors of Nursing to lead the clinical programs in our operations. Working together with their operational CEO and/or administrator, other key operational leaders and front-line staff, these experienced nurses manage delivery of care and other clinical personnel and programs to optimize both clinical outcomes and employee and patient satisfaction.
Increase Mix of High Acuity Patients — Many skilled nursing facilities are serving an increasingly larger population of patients who require a high level of skilled nursing and rehabilitative care, whom we refer to as high acuity patients, as a result of government and other payors seeking lower-cost alternatives to traditional acute-care hospitals. We generally receive higher reimbursement rates for providing care for these medically complex patients. In addition, many of these patients require therapy and other rehabilitative services, which we are able to provide as part of our integrated service offerings. Where higher complex services are medically necessary and prescribed by a patient's physician or other appropriate healthcare professional, we generally receive additional revenue in connection with the provision of those services. By making these integrated services available to such patients, and maintaining established clinical standards in the delivery of those services, we are able to increase our overall revenues. We believe that we can continue to attract high acuity patients to our operations by maintaining and enhancing our reputation for quality care and continuing our community focused approach.
12
Focus on Organic Growth and Internal Operating Efficiencies — We plan to continue to grow organically by focusing on increasing patient occupancy within our existing operations. Although some of the facilities we have acquired were in good physical and operating condition, the majority have been clinically and financially troubled, with some facilities having had occupancy rates as low as 30% at the time of acquisition. Additionally, we believe that incremental operating margins on the last 20% of our beds/units are significantly higher than on the first 80%, offering opportunities to improve financial performance within our existing facilities. Our overall occupancy is impacted significantly by the number of facilities acquired and the operational occupancy on the acquisition date. Therefore, consolidated occupancy will vary significantly based on these factors. Our average occupancy rates for our skilled nursing facilities was 75.3% and 72.8% for the years ended December 31, 2022 and 2021, respectively. Our average occupancy rates in 2022 continue to improve as we recover from the COVID-19 pandemic.
We also believe we can generate organic growth by improving operating efficiencies and the quality of care at the patient level. By focusing on staff development, clinical systems and the efficient delivery of quality patient care, we believe we are able to deliver higher quality care at lower costs than many of our competitors.
Historically, we have achieved incremental occupancy and revenue growth by creating or expanding clinical service offerings in existing operations. For example, by expanding clinical programs to provide outpatient therapy services in many markets, we are able to increase revenue while spreading the fixed costs of maintaining these programs over a larger patient base. Outpatient therapy has also proven to be an effective marketing tool, raising the visibility of our facilities in their local communities and enhancing the reputation of our facilities with short-stay rehabilitation patients.
Add New Facilities and Expand Existing Facilities — One of our growth strategies includes the acquisition of new and existing facilities from third parties and the expansion and upgrades to current facilities. In the near term, we plan to take advantage of the fragmented skilled nursing industry by acquiring operations within select geographic markets and may consider the construction of new facilities. In addition, we have targeted facilities that we believed were performing and operations that were underperforming, where we believed we could improve service delivery, occupancy rates and cash flow. With experienced leaders in place at the community level and demonstrated success in significantly improving operating conditions at acquired facilities, we believe that we are well positioned for continued growth. While the integration of underperforming facilities generally has a negative short-term effect on overall operating margins, these facilities are typically accretive to earnings within 12 to 18 months following their acquisition. For the facilities that we acquired from 2001 through 2022, the aggregate EBITDAR as a percentage of revenue improved from 15.8% during the first full three months of operations to 17.2% during the thirteenth through fifteenth months of operation and to 18.8% during the 45th quarter of operation.
Standard Bearer Portfolio Growth — An important part of our business strategy is to continue to expand and diversify our real estate portfolio through accretive acquisition and investment opportunities in healthcare properties. Our execution of this strategy hinges on our ability to successfully identify, secure and consummate beneficial transactions. We have a proven track record of acquiring properties that we have determined are investment opportunities and develop these into thriving properties that are well-suited for operational purposes. We then use these properties for our skilled nursing or senior living operations, or we lease the properties to other long-term care facility operators. We expect that our newly formed REIT structure will allow us to expand our real estate footprint while bringing the best operational practices to our own and other operators in the industry.
HUMAN CAPITAL
At December 31, 2022, we had approximately 29,900 full-time equivalent employees who were employed by our Service Center and our operating subsidiaries. For the year ended December 31, 2022, approximately 60.0% of our total expenses were payroll related. Periodically, market forces, which vary by region, require that we increase wages in excess of general inflation or in excess of increases in reimbursement rates we receive. We believe that we staff appropriately, focusing primarily on the acuity level and day-to-day needs of our patients and residents. In most of the states where we operate, our skilled nursing facilities are subject to state mandated minimum staffing ratios, so our ability to reduce costs by decreasing staff, notwithstanding decreases in acuity or need, is limited and subject to government audits and penalties in some states. We seek to manage our labor costs by improving staff retention, improving operating efficiencies, maintaining competitive wage rates and benefits and reducing reliance on overtime compensation and temporary nursing agency services. Our Chief Human Capital Officer reports to our Board of Directors and oversees the following human capital initiatives:
13
Our Culture — The operation of our skilled nursing and senior living facilities requires a large number of highly skilled healthcare professionals and support staff. Our employees are at the heart of our Company and we are committed to their health, professional development and workplace satisfaction. Our core values, which focuses on developing our employees, fostering an ownership mentality and allowing for intelligent risk taking, guide us in our decision making and inspire us to be better people, both professionally and personally.
Compensation and Benefits — The healthcare industry as a whole has been experiencing shortages of qualified professional clinical staff. We believe that our ability to attract and retain qualified professional clinical staff stems from our ability to offer attractive wage and benefits packages, a high level of employee training, an empowered culture that provides incentives for individual efforts and a quality work environment.
Diversity and Inclusion — We value diversity in our recruiting, hiring and career development practices. Our commitment is to provide equal opportunity and fair treatment to all individuals based on merit and without discriminations. In 2022, we formed our Diversity, Equity and Inclusion (DEI) Committee, a multidisciplinary group led by our Chief Executive Officer, to advance our DEI initiatives throughout the organization
Training and Development — We provide training and development to all employees. We have many training programs at all levels such as our CEO in Training, Director of Nursing in Training, Director of Rehab in Training, nursing certified assistant schools, weekly culture trainings, boot camps and annual meetings, where we focus on both career and professional development.
Social Sustainability — We continuously work towards bridging the gap between what the healthcare system currently provides and the basic needs of individuals. We aim to have an enduring impact on the communities in which we live and work. Elevate Charities is a non-profit organization that is dedicated to elevating the condition and quality of life for members of the senior healthcare community - employees, caregivers, family members, patients and residents. Elevate Charities has three unique funds: Heritage Fund, Heritage Scholarship Fund and the Emergency Fund.
The Heritage Fund and the Heritage Scholarship Fund engage in a mission to enhance the quality of life for seniors in our communities through caring service, fulfilling essential needs and providing education to caregivers. The Heritage Fund helps the caregiver identify specific and practical ways to meet the needs of those under their care. This can help provide a better life, improved experience and greater satisfaction for our aging population. The financial support provided by the Heritage Fund benefits seniors directly. In addition, the Heritage Scholarship Fund helps qualified clinical professionals who may not be able to afford to advance in the field of long-term care. Through grants and scholarships, the fund helps these qualified professionals gain the education needed to advance in the field of senior-focused healthcare. Since 2019, we awarded 150 scholarships to employees in our workforce.
Lastly, the Emergency Fund is a way of passing the hat to help our co-workers whose lives are affected by tragedy. This program is funded for Company team members by the Company team members. All Company team members can contribute to the fund either through a one-time donation or by recurring payroll deduction. In 2022, approximately 80% of those employed by our operating subsidiaries contributed to the Emergency Fund. In 2022, we distributed approximately $2.5 million in grants to members of our Ensign-affiliated family. To date, the Emergency Fund has distributed over 10,900 grants totaling almost $12.5 million to members of our Ensign-affiliated family in their time of need.
COVID-19 — Our teams have been on the front lines in the battle against COVID-19. When it would have been easier to simply hunker down and wait for the challenges to pass, the heroes in our operations continued to provide selfless service to all their patients, including COVID patients. To recognize these front-line workers, our company, along with each individual operating subsidiary, provided financial awards to our employees for their tirelessly daily efforts to provide outstanding care to each resident they serve. We are beyond grateful for their enormous efforts and will continue to recognize the sacrifices of these employees as we navigate through the pandemic.
For additional information on human capital matters, please see our most recent proxy statement or Environmental, Social and Governance (ESG) report, each of which is available on our website at www.ensigngroup.net. For additional information on Elevate Charities, please visit www.elevatecharities.org. The information contained in, or that can be accessed through, either of the foregoing websites does not constitute a part of this Annual Report on Form 10-K.
14
GOVERNMENT REGULATION
General
Healthcare is an area of extensive and frequent regulatory change. Changes in the law or new interpretations of existing laws may have a significant impact on revenue, costs and business operations. Our independent operating subsidiaries that provide healthcare services are subject to federal, state and local laws relating to, among other things, licensure, quality and adequacy of care, physical plant requirements, life safety, personnel and operating policies. In addition, these same subsidiaries are subject to federal and state laws that govern billing and reimbursement, relationships with vendors, business relationships with physicians and workplace protection for healthcare staff. Such laws include the Anti-Kickback Statute (AKS), the federal False Claims Act (FCA), the Stark Law, the Health Care Emergency Temporary Standard and state corporate practice of medicine statutes.
Governmental and other authorities periodically inspect the skilled nursing facilities (SNFs), senior living facilities and outpatient rehabilitation agencies of our independent operating subsidiaries to verify continued compliance with applicable regulations and standards. The operations must pass these inspections to remain licensed under state laws and to comply with Medicare and Medicaid provider agreements. The operations can only participate in these third-party payment programs if inspections by regulatory authorities reveal that the operations are in substantial compliance with applicable state and federal requirements. In the ordinary course of business, federal or state regulatory authorities may issue notices to the operations alleging deficiencies in certain regulatory practices. These statements of deficiency may require corrective action to regain and maintain compliance. In some cases, federal or state regulators may impose other remedies including imposition of civil monetary penalties, temporary payment bans, loss of certification as a provider in the Medicare or Medicaid program, or revocation of a state operating license.
We believe that the regulatory environment surrounding the healthcare industry subjects providers to intense scrutiny. In the ordinary course of business, providers are subject to inquiries, investigations and audits by federal and state agencies related to compliance with participation and payment rules under government payment programs. These inquiries may originate from the United States Department of Health and Human Services (HHS) Office of the Inspector General (OIG), state Medicaid agencies, state Attorney Generals, local and state ombudsman offices and CMS Recovery Audit Contractors, among other agencies. In response to the inquiries, investigations and audits, federal and state agencies continue to impose citations for regulatory deficiencies and other regulatory penalties, including demands for refund of overpayments, expanded civil monetary penalties that extend over long periods of time and date back to incidents prior to surveyor visits, Medicare and Medicaid payment bans and terminations from the Medicare and Medicaid programs, which may be temporary or permanent in nature. We vigorously contest each such regulatory outcome when appropriate; however, there are significant legal and other expenses involved that consume our financial and personnel resources. Expansion of enforcement activity could adversely affect our business, financial condition or the results of operations.
Coronavirus
In an effort to promote efficient care delivery and to decrease the spread of COVID-19, federal, state and local regulators have implemented new regulations and waived (in some cases, temporarily) certain existing regulations, including those set forth below, which may expire in 2023.
Temporary suspension of certain patient coverage criteria and documentation and care requirements — The Coronavirus Aid, Relief and Economic Security Act of 2020 (the CARES Act) and a series of temporary waivers and guidance issued by CMS suspended various Medicare patient coverage criteria to ensure patients continue to have adequate access to care, notwithstanding the burdens placed on healthcare providers as related to the COVID-19 pandemic. Many of these regulatory waivers were issued pursuant to Section 1135 of the Social Security Act, which authorizes the HHS Secretary to temporarily waive or modify Medicare and Medicaid requirements for affected health care providers and facilities following the declaration of a Public Health Emergency (PHE). HHS also waived requirements specific to SNFs.
Pursuant to the Emergency Waivers, CMS also authorized temporary waivers on medical review requirements, effective March 1, 2020. In addition, CMS also downgraded the priority for scheduled program audits and contract-level Risk Adjustment Data Validation audits for Medicare Advantage organizations, Part D sponsors, Medicare-Medicaid Plans and Programs of All-Inclusive Care for the Elderly organizations. Reducing the priority of those standard or scheduled audit activities allows providers, CMS and other organizations to focus on patient care, including directing audit activities toward infection control. The reprioritization of its audit activities was time-limited and normal activities resumed in 2022, including the expiration of certain Emergency Waivers.
15
Beginning on May 7, 2021, CMS started to end certain Emergency Waivers related to the COVID-19 pandemic, beginning with waivers regarding data reporting and resident grouping, transfer and discharge. The expiration of additional Emergency Waivers in place for SNF and long-term care (LTC) facilities, along with the expiration of other Emergency Waivers for other residential facilities other than hospitals and critical access hospitals occurred on June 6, 2022.
The first group of seven Emergency Waivers that expired on May 7, 2022 were: (1) waiver of the requirement that residents participate in-person during resident groups; (2) physicians’ ability to delegate tasks that otherwise would need to be personally performed by a physician within a SNF; (3) waiver of the requirement for physicians to make personal visits to patients, which the Emergency Waivers allow physicians to delegate to other clinicians; (4) waiver of the requirement for physicians and non-physician providers to conduct in-person visits to nursing home residents (and allowing those visits to be made via telemedicine as appropriate); (5) reducing LTC facilities’ requirements to develop, implement and maintain a Quality Assurance and Performance Improvement (QAPI) program that satisfies federal standards; (6) waiver of LTC facilities’ obligation to participate in discharge planning for residents ending their care at the facility; and (7) waiver of the requirement for LTC facilities to provide residents with a copy of their records within two working days of a resident’s request for those records.
The Emergency Waivers that expired on June 6, 2022 were: (1) waivers of SNF physical environment conditions for temporary use facilities (including COVID-19 treatment locations) and use of interior or non-residential space within a SNF to accommodate residents; (2) waivers of requirements for timely preventative maintenance for certain equipment, including dialysis equipment; (3) the waiver of inspection, testing and maintenance for the facilities and medical equipment used within ICFs and SNFs; (4) the waiver of inspection, testing and maintenance for compliance with applicable life safety codes and health care facility codes for intermediate care facilities (ICFs) and SNFs; (5) the waiver of CMS’s requirement for ICFs and SNFs to have an exterior door or window in every room used for sleeping; (6) life safety code waivers of quarterly fire drills and allowing SNFs to erect temporary walls and barriers between patients; (7) waiving CMS’s minimum training requirements for paid feeding assistants in LTC facilities; (8) CMS’s waiver of its requirement for nurse aides within SNFs to receive at least 12 hours of annual in-service training; and (9) the waiver of an SNF’s normal obligation not to employ any nursing aid longer than 4 months if he or she does not satisfy federal training and certification requirements.
CMS may terminate other Emergency Waivers affecting SNF and other LTC facilities in the future and these terminations may occur quickly and with little public notice. Due to the prevalence of waves of COVID-19 variants, it is uncertain when the remaining Emergency Waivers will expire.
Examples of the Emergency Waivers still in effect as of December 31, 2022 include, but are not limited to, the following: (1) approving temporary transfer, discharge and cohorting of patients to ensure that facilities can separate COVID-19 negative patients from those that are positive for or have been exposed to the virus; (2) allowing SNFs to provide a skill-in-place program for Medicare beneficiaries who are residents of the SNF that meet the skill-in-place criteria, foregoing the usual three-day qualifying hospital stay; and (3) temporarily waiving certain documentation and reporting requirements regarding patient admission, transfer and discharge. Some States have also waived regulations to ease regulatory burdens on the healthcare industry. It remains uncertain when federal and state regulators will resume enforcement of those regulations, which remain waived or are otherwise not being enforced during the PHE. We believe these regulatory actions could contribute to changes in skilled mix, which may have been different without the existence of the Emergency Waivers.
Resuming visitation and resident rights — CMS has issued guidance to facilities throughout the PHE regarding patients’ rights to visitation. While the CMS guidance issued in March 2020 directed facilities to severely restrict visitation, CMS subsequently provided and updated guidance through the course of the pandemic that broadens visitation and provides guidance on visitation procedures. On September 23, 2022, CMS updated their visitation guidance to recommend the use of masks or face coverings when the county where the facility is located has a high rate of COVID-19 transmission, encouraged the use of masks or face coverings regardless of COVID-19 transmission status and allows residents and visitors to choose not to wear masks or face coverings when alone in the resident's room or in a dedicated visitation area. This most recent CMS guidance also included updated advice related to isolation of known or suspected positive COVID-19 cases or those exposed to positive COVID-19 cases. The guidance also encouraged distancing during large group gatherings within the facility.
16
Testing requirements — Beginning in April 2020, authorities in several states in which our independent operating subsidiaries are located began to mandate widespread COVID-19 testing at all nursing home and LTC facilities. This came after the Centers for Disease Control and Prevention (CDC) stated that older adults are at a higher risk for serious illness from the coronavirus and issued updated testing guidelines for nursing homes. Some of these states were also publicly reporting COVID-19 outbreaks in facilities. On April 27, 2021, CMS issued revised parameters for testing, specifying that the requirement for routine testing of staff applies only to those staff members that are unvaccinated - fully vaccinated staff do not have to be routinely tested. Thereafter, CMS's interim final rule (IFR) regarding COVID-19 testing of staff, released on September 23, 2022 stated that routine testing of staff for COVID-19 is no longer generally recommended without exposure to COVID-19. This guidance clarified that individuals who show symptoms of COVID-19, regardless of vaccination status, should be tested for COVID-19 as soon as possible. Additionally, this IFR called for testing of residents and staff and investigation of an outbreak when there is a single positive COVID-19 case among residents or staff of the LTC facility.
Federal and state COVID-19 vaccination requirements — As the Pfizer, Moderna, Johnson & Johnson and Novavax vaccines received FDA approval, CMS developed an IFR requiring all workers within Medicare and Medicaid-participating nursing homes to be vaccinated against COVID-19 as a condition of participation in the Medicare and Medicaid programs. In addition, OSHA introduced an emergency temporary standard (ETS) requiring employers with more than 100 employees to mandate that its employees be fully vaccinated against COVID-19 or submit to weekly testing for the virus. Both CMS’s IFR and OSHA’s emergency temporary standard (ETS) for vaccination were challenged in court and halted from enforcement in certain states, but the United States Supreme Court allowed CMS to enforce its vaccine mandate nationwide.
In addition to the IFR mandating vaccinations for health facility workers, several states where our independent operating facilities are located have issued vaccine mandates that apply to facility staff. These vaccine mandates are largely aligned with CMS's requirements. For example, California issued an order requiring adult care facilities and direct care workers to be vaccinated as well, and for all affected workers to be fully vaccinated by November 30, 2021. The order was expanded to allow workers who had completed their primary vaccination series and contracted COVID-19 since becoming fully vaccinated to defer the receipt of a vaccine booster dose by up to 90 days after infection with COVID-19; otherwise, booster vaccine doses were required to be completed by March 1, 2022. On October 23, 2022, CMS issued further guidance unifying its recommendations for all facilities under its oversight, including SNFs and LTC facilities, reaffirming CMS's activities to verify vaccination of all SNF and LTC facility staff, and where necessary, to pursue corrective action for facilities found deficient in this requirement.
Reporting requirements — In accordance with CMS reporting guidance, SNFs are required to report to the CDC National Health Safety Network certain information related to COVID-19 cases on a weekly basis. Facilities are also required to provide residents and staff with vaccine education and offer vaccines, when available, to residents and staff. The IFR published on August 23, 2021 requires facilities to develop policies and procedures to ensure the availability of the COVID-19 vaccine to residents and staff and to educate them concerning the benefits, risks and potential side effects associated with the vaccine. CMS may initiate enforcement activities and assess civil monetary penalties for not meeting any of these COVID-19 related reporting requirements under this IFR and reaffirmed its intent to seek corrective action against SNFs and LTC facilities that do not satisfy these requirements. We do not believe these COVID-19 related requirements will have a material impact on our consolidated financial statements.
Survey Activity and Enforcement — In response to the COVID-19 pandemic environment, CMS included infection controls as part of its survey process along with updating its patients' and residents' rights to receive visitor guidance. The spectrum of remedies available to CMS for imposition includes increased monetary fines, shortened time periods to return to compliance and other administrative penalties for deficiencies.
Changes to Medicaid Reimbursement — In March of 2020, the Families First Coronavirus Relief Act (FFCRA) provided a 6.2% increase to the Federal Medicaid Assistance Percentage (FMAP) during the PHE. In addition to this funding increase, the FFCRA imposed conditions restricting the disenrollment and standards for re-enrolling Medicaid beneficiaries to promote continuous care of beneficiaries during the PHE. The bipartisan omnibus spending plan passed by Congress and signed into law by the President on December 29, 2022, amended these Medicaid enrollment protections and increased FMAP funding provided in the FFCRA. In the first quarter of 2023 the FMAP increase CMS provides to the States will remain elevated by 6.2%, but will decline for the remaining quarters in 2023, subject to further reductions noted below: for the second quarter, April through June 2023, this increase will be reduced to 5%; in the third quarter, from July through September, the FMAP increase will be reduced to 2.5%, and in October through December, the FMAP increase will be reduced to 1.5%. Previously, the FMAP funding was dependent on the termination of the PHE. The ultimate amount of funding from each state will vary substantially based on that states’ policies.
17
CMS’s provision of these increased FMAP funds to states is conditioned upon states reporting to CMS certain Medicaid-related information, including data pertaining to Medicaid renewals, termination of Medicaid coverage, beneficiary customer service information, and other eligibility and renewal information that may be identified in regulations or by the HHS Secretary. States that do not report required data to CMS beginning in July of 2023 will be penalized .25 percentage points, up to a total of one percentage point, for each quarter the state does not report data to CMS. The omnibus spending plan also grants CMS authority to impose fines, penalties, and other sanctions upon states that do not comply with this law’s requirements for the unwinding of increased FMAP payments.
Under the omnibus spending bill adopted in December of 2022, states may begin disenrolling Medicaid beneficiaries beginning on April 1, 2023. The FFCRA contemplated continuous Medicaid enrollment until the end of the PHE and provided funding for enrollment during that duration. The omnibus spending plan winds down this Medicaid spending for continuous enrollment in phases, ultimately reducing CMS’s contribution to state-administered Medicaid programs. CMS guidance permits states up to 14 months to initiate and process traditional Medicaid renewals, including the eligibility and enrollment process.
Medicare
Medicare presently accounts for approximately 28.6% of our skilled nursing services revenue year-to-date, being our second-largest payor. The Medicare program and its reimbursement rates and rules are subject to frequent change. These include statutory and regulatory changes, rate adjustments (including retroactive adjustments), administrative or executive orders and government funding restrictions, all of which may materially adversely affect the rates at which Medicare reimburses us for our services. Budget pressures often lead the federal government to reduce or place limits on reimbursement rates under Medicare. Implementation of these and other types of measures has in the past, and could in the future, result in substantial reductions in our revenue and operating margins.
Patient-Driven Payment Model (PDPM)
The Skilled Nursing Facility Prospective Payment System (SNF PPS) Rule became effective October 1, 2019. The SNF PPS Rule includes a new case-mix model that focuses on the patient’s condition (clinically relevant factors) and resulting care needs, rather than on the volume of care provided, to determine Medicare reimbursement. The case mix-model is called the Patient-Driven Payment Model (PDPM), which utilizes clinically relevant factors for determining Medicare payment by using International Classification of Diseases, Tenth Revision diagnosis codes and other patient characteristics as the basis for patient classification. PDPM utilizes five case-mix adjusted payment components: physician therapy, occupational therapy, speech language pathology, nursing and social services and non-therapy ancillary services. It also uses a sixth non-case mix component to cover utilization of SNFs' resources that do not vary depending on resident characteristics.
PDPM replaces the existing case-mix classification methodology, Resource Utilization Groups, Version IV. The structure of PDPM moves Medicare towards a more value-based, unified post-acute care payment system. For example, PDPM adjusts Medicare payments based on each aspect of a resident’s care, thereby more accurately addressing costs associated with medically complex patients. PDPM also removes therapy minutes as the basis for therapy payment. Finally, PDPM adjusts the SNFs' per diem payments to reflect varying costs throughout the stay, through the physician therapy, occupational therapy and non-therapy ancillary services components.
In addition, PDPM is intended to reduce paperwork requirements for performing patient assessments. Under the SNF PPS PDPM system, the payment to SNFs and nursing homes is based heavily on the patient’s condition rather than the specific services provided by each SNF.
Skilled Nursing Facility - Quality Reporting Program (SNF QRP)
The Improving Medicare Post-Acute Care Transformation Act of 2014 (IMPACT Act) provided data reporting requirements for certain Post-Acute-Care (PAC) providers. The IMPACT Act requires that each SNF submit their quality measures data. If a SNF does not submit required quality data, their payment rates are reduced by 2.0% for each such fiscal year. Application of the 2.0% reduction may result in payment rates for a fiscal year being less than the preceding fiscal year. In addition, reporting-based reductions to the market basket increase factor will not be cumulative; they will only apply for the fiscal year involved. A SNF's Medicare Administrative Contractor will issue the facility a notice of non-compliance if it does not satisfy its Quality Reporting Program (QPR) reporting requirements.
The SNF QRP standardized a number of standardized patient assessment data elements. The SNF QRP applies to freestanding SNFs, SNFs affiliated with acute care facilities and all non-critical access hospital swing-bed rural hospitals.
18
On July 29, 2021, two new reporting measures were required under the SNF QRP. Starting with the FY 2023 SNF QRP, SNFs are required for the first time to report the SNF Healthcare-Associated Infections (HAI) measure, which tracks the number of infections requiring hospitalization following a medical intervention, and the COVID-19 Vaccination Coverage among Healthcare Personnel (HCP) measure, which tracks COVID-19 vaccination of staff in order to assess whether SNFs are taking steps to limit the spread of COVID-19. The Transfer of Healthcare (TOH) information data SNFs must report, which is included in the Patient-Post-Acute Care measurement, will be changed to exclude SNF patients discharged to their homes under the care of either a home health service or hospice. The elimination of this information will change how the TOH is used in calculating Patient-Post-Acute Care measurement, and may have an impact on our quality ratings and reimbursement from Medicare and Medicaid on a prospective basis.
Beginning in March 2020, due to the COVID-19 pandemic, CMS issued a temporary suspension of SNF QRP reporting requirements effective until June 30, 2020. This effectively gave SNFs discretion as to whether to report data from the fourth quarter (October 1, 2019 – December 31, 2019), and removed reporting requirements entirely for the first and second quarters of 2020 (January 1, 2020 – June 30, 2020). SNFs were required to resume timely quality data collection and submission of measure and patient assessment data effective June 30, 2020. In January 2022, SNF ratings based on the resumed data reporting were recalculated for publication.
In July of 2022, CMS announced revisions to calculating its five-star ratings for the Nursing Home Compare website. Under this new calculation, points are assigned to a SNF based on its performance across six measures: (1) case-mix adjusted total nurse staffing levels (including registered nurses, licensed practical nurses, and nursing aides), measured by hours per resident per day; (2) case-mix adjusted registered nurse staffing levels, measured by hours per resident per day; (3) case-mix adjusted total nurse staffing levels (including registered nurses, licensed practical nurses, and nursing aides), measured by hours per resident day on the weekend; (4) total nurse turnover, defined as the percentage of nursing staff that left the nursing home over a 12-month period; (5) registered nurse turnover, defined as the percentage of registered nursing staff that left the nursing home over a 12-month period; and (6) administrator turnover, defined as the percentage of administrators that left the nursing home over a 12-month period. These six measures will be measured on a quarterly basis.
Staff measurements are scored based on the points assigned to these six measures. For case-mix adjusted total nurse staffing and case-mix adjusted registered nurse staffing, each measure is scored on a 100-point scale in 10-point increments. For case-mix adjusted total nurse staffing on weekends, total nurse turnover, and total registered nurse turnover, each measure is scored on a 50-point scale in five-point increments. The measure of administrator turnover is measured on a 30-point scale, with points assigned based on the number of administrator departures during the measurement period. The result of these staffing measures will affect a SNF’s total five-star score reported on the Nursing Home Compare website.
These six new measures were included in the five-star rating in October 2022 in addition to other changes. In addition, CMS also implemented a planned increase to the quality measure reporting thresholds, increasing each threshold by one-half of the average improvement of quality measure scores since CMS last set quality measure thresholds. Going forward, CMS plans to implement similar rating threshold increases every six months.
On July 29, 2022, CMS announced the adoption of a process measure for influenza vaccination coverage among healthcare personnel within SNFs. This measure will be determined by the percentage of SNF healthcare personnel who receive an influenza vaccine any time from when it first becomes available through March 31 of the following year. SNFs began submitting this data on October 1, 2022 through March 31, 2023.
Additionally, CMS revised certain SNF data reporting requirements, including the transfer of health information measures and certain patient assessment data elements, including ethnicity, preferred language, health literacy, and social isolation, until October 1, 2023.
Medicare Annual Payment Rule
CMS is required to calculate an annual Medicare market-basket update to the payment rates. On July 29, 2022, CMS issued a final rule for fiscal year 2023 that updates the Medicare payment rates to aggregate net market basket increased by 2.7%. The increase is resulted from the 5.1% update to the market basket, which is based on a 3.9% current year market basket increase plus a 1.5% market basket error adjustment, less a 0.3% productivity adjustment and a negative 2.3% adjustment as a result of the recalibrated parity adjustment. The recalibrated parity adjustment is being phased in at a rate of 2.3% per year over two years.
19
On July 29, 2021, CMS issued a final rule for fiscal year 2022 that updates the Medicare payment rates and the quality programs for SNFs. Under the final rule, effective October 1, 2021, the aggregate net market basket rate increased by 1.2% for fiscal year 2022, compared to fiscal year 2021. This increase is attributable to a 2.7% market basket increase factor with a 0.8% reduction for forecast error adjustment and a 0.7% reduction for multifactor productivity adjustment.
Sequestration of Medicare Rates
The Budget Control Act of 2011 requires a mandatory, across the board reduction in federal spending, called a sequestration. Medicare FFS claims with dates of service or dates of discharge on or after April 1, 2013 incur a 2.0% reduction in Medicare payments. All Medicare rate payments and settlements have incurred this mandatory reduction and will continue to be in place through at least 2023, unless Congress takes further action. In response to COVID-19, the CARES Act temporarily suspended the automatic 2.0% reduction of Medicare claim reimbursements for the period of May 1, 2020 through December 31, 2020. On December 27, 2020, the Consolidated Appropriations Act further suspended the 2.0% payment adjustment through March 31, 2021. On April 14, 2021, Congress extended the suspension of the 2.0% payment adjustment through December 31, 2021. On December 10, 2021, President Biden signed into law a bill to postpone the 2.0% payment adjustment through April 1, 2022; from April 1, 2022 through June 30, 2022, the 2.0% payment adjustment is reduced from 2.0% to 1.0%. To pay for the change, Congress would increase the sequester cuts by one year to fiscal year 2030. As of July 1, 2022, Medicare's sequestration cuts have reverted to 2%, which was the sequestration rate in effect before the COVID-19 PHE commenced.
Skilled Nursing Facility Value-Based Purchasing (SNF-VBP) Program
The SNF-VBP Program rewards SNFs with incentive payments based on the quality of care they provide to Medicare beneficiaries, as measured by a hospital readmissions measure. CMS annually adjusts its payment rules for SNFs using the SNF-VBP Program. To fund the SNF-VBP Program incentive payment pool, CMS withheld 2% of Medicare payments and will redistribute 60% of the withheld payments back to SNFs through the program. The program also introduced quality measures to assess how health information is shared and adopted a number of standardized patient assessment data elements that assess factors such as cognitive function and mental status, special services and social determinants of health. On July 29, 2021, CMS finalized its changes for measuring the performance period and amending the data to be reported to CMS, which impacted the SNF-VBP Program rate adjustment to account for COVID-19 impacting readmission rates and SNF admissions during the performance periods of fiscal year 2020. The deadlines for baseline period quality measure quarterly reporting and performance periods and standards will start in the 2023 program year.
On July 29, 2022, CMS released the final rule electing to not apply the SNF 30-Day All-Cause Readmission Measure (SNFRM) as part of performance scoring for fiscal year 2023. CMS will still publicly report the SNFRM, but it will not affect SNF payments. The final rule for the fiscal year 2023 SNF PPS also provided for SNF-VBP program expansion beyond the use of its single, all-cause hospital readmission measure to determine payment, with the inclusion of measures in fiscal year 2026 for SNF healthcare associated infections requiring hospitalization (SNF HAI) and total nursing hours per resident day measures, and in fiscal year 2027, the discharge to community post acute care measure for SNFs, which assesses the rate of successful discharges to the community from a SNF setting.
On February 28, 2022, the Administration published a fact sheet stating its priorities for making changes to senior care, including potential changes to regulations affecting LTCs and SNFs. The SNF-VBP Program was identified as an area for change, with staffing levels, retention and resident experience affecting reimbursement. Following studies by CMS, proposed rules that may affect the SNF-VBP Program are expected by early 2023, with final rules to follow after a notice-and-comment period.
20
Part B Rehabilitation Requirements
Some of our revenue is paid by the Medicare Part B program under a fee schedule. Part B services are limited with a payment cap by combined speech-language pathology services (SLP), physical therapy (PT) services and a separate annual cap for occupational therapy (OT) services. These caps were implemented under the authority of the Balanced Budget Amendments of 1997. These amounts were previously associated with the financial limitation amounts. The Bipartisan Budget Act of 2018 (BBA) repealed those caps while retaining and adding additional limitations to ensure appropriate therapy services. This policy does not limit the amount of medically necessary Medicare Part B therapy services a beneficiary may receive. The BBA establishes coding modifier requirements to obtain payments beyond the updated KX modifier thresholds, discussed below, and reaffirms the specific $3,000 claim audit threshold requirements for the Medicare Administrative Contractors. For PT and SLP combined the threshold for coding modifier requirements was $2,110 for 2021. The KX Modifier threshold was set at $2,150 for CY 2022 with the same threshold for OT services. For CY 2023, the KX modifier threshold has been increased by 3.8%, to $2,230 for PT and SLP, with the same threshold for OT services as well. The KX modifier is a modifier added to medical claims to indicate the providing clinician attests that the services corresponding to that claim were medically necessary and that the justification for those services is contained within the patient’s medical records. This modifier is intended for use where the services will exceed the threshold for those services set by the BBA and updated by annual fee schedule rules, yet are still appropriate and medically necessary, and thus should be compensated by Medicare.
Consistent with CMS’s “Patients over Paperwork” initiative, the agency has also been moving toward eliminating burdensome claims-based functional reporting requirements. Beginning in 2021, CMS rescinded 21 problematic National Correct Coding Initiative edits impacting outpatient therapy services, including services furnished under Medicare Part B primarily related to PT and OT services, removing a coding burden caused by requirements for additional documentation and claim modifier coding.
The calendar year 2021 Physician Fee Schedule (PFS) Final Rule reduced the conversion factor (i.e. the number by which CMS determine all current procedural terminology code payments) by 10.2%. These changes lowered the reimbursement rate for therapy Medicare Part B specialty providers by 9% for PT and OT and by 6% for SLP codes. These reductions were mitigated by the Consolidated Appropriations Act of 2021 (CAA, also referred to as The Omnibus Appropriations Law). The CAA includes three components relevant to the Medicare Part B PFS. First, the CAA incorporated a rate relief of approximately 3.75% for fiscal year 2021. Additionally, the CAA incorporated a freeze to the payment for the physician add-on code for three years which would effectively create relief on the initial cuts through 2023. Finally, the relief called for the 2% sequester to not be applied to the Medicare Part B program for the first quarter of 2021. In addition, the 2% sequester was suspended.
The calendar year 2022 PFS (2022 PFS) required the use of new modifiers to identify and make payments at 85% of the otherwise applicable Part B payment amount for PT and OT services furnished in whole, or in part by PT and OT assistants. The 2022 PFS resulted in FFS Medicare payments adjusted by a sequester of 1% from April 1, 2022 through June 30, 2022, and further adjusted by a total of 2% from July 1, 2022 through December 31, 2022.
On November 1, 2022, CMS issued the calendar year 2023 PFS that would result in a PFS conversion factor of $33.06, a decrease of $1.55 from the calendar year 2022 PFS conversion factor of $34.61. This is a 4.47% cut to the conversion factor for calendar year 2023.
The Multiple Procedure Payment Reduction (MPPR) continues at a 50% reduction, which is applied to therapy procedures by reducing payments for practice expense of the second and subsequent procedures when services provided beyond one unit of one procedure are provided on the same day. The implementation of MPPR includes (1) facilities that provide Medicare Part B speech-language pathology, occupational therapy and physical therapy services and bill under the same provider number; and (2) providers in private practice, including speech-language pathologists, who perform and bill for multiple services in a single day.
21
On May 27, 2020, pursuant to its authority under the Emergency Waivers, CMS added physical therapy, occupational therapy and speech-language pathology to the list of approved telehealth Providers for the Medicare Part B programs provided by a SNF. Subsequently, the calendar year 2021 and 2022 PFS Final Rules added certain of these PT and OT services to the list of Medicare telehealth services on a temporary basis through at least the end of calendar year 2023. On December 31, 2020, CMS announced its 2021 update to the list of codes that describe Medicare Part B outpatient therapy services, making permanent existing and new codes introduced during the COVID-19 PHE for use under PT, OT, or SLP, including several telehealth codes as “sometimes therapy,” to permit physicians and certain non-physician practitioners to render these services outside a therapy plan of care when appropriate. “Sometimes therapy” codes will not have the MPPR applied. On November 19, 2021, CMS expanded these “sometimes therapy” codes further for the 2022 PFS, including five new codes for remote therapeutic monitoring treatment, which are broader than pre-existing monitoring codes and include measuring and evaluating adherence and response to medication and therapy. The Emergency Waivers allow therapists to bill Telehealth therapy services up to 151 days after the end of the PHE.
Pursuant to the Emergency Waivers, CMS allowed for the facility to bill an originating site fee to CMS for telehealth services provided to Medicare Part B beneficiary residents of the facility when the services were provided by a physician from an alternate location, effective March 6, 2020 and ending on May 7, 2022. Our Facilities have thus ceased using these telemedicine Emergency Waivers upon their termination.
Programs of All-Inclusive Care for the Elderly
The requirements under the Programs of All-Inclusive Care for the Elderly (PACE) provide greater operational flexibility and update information under the Medicare and Medicaid programs. Such flexibility includes: (i) more lenient standards applicable to the current requirement that the PACE organization be monitored for compliance with the PACE program requirements during and after a 3-year trial period and (ii) relieving certain restrictions placed upon the interdisciplinary team that comprehensively assesses and provides for the individual needs of each PACE participant by allowing one person to fill two roles and permitting secondary participation in the PACE program. Further, non-physician primary care providers can provide certain services in place of primary care physicians. On October 21, 2021, CMS published an extension of the timeline to complete further final rulemaking for the PACE program until November 1, 2022, which focuses on policy and technical changes to Medicare Advantage, Medicare Prescription Drug Benefit, PACE, Medicaid FFS and Medicaid managed care programs. On November 2, 2022, CMS further extended the timeline for issuing its final rule for the PACE program by three months, until February 1, 2023.
Decisions Regarding Skilled Nursing Facility Payment
Medicare reimbursement rates and rules are subject to frequent change. Historically, adjustments to reimbursement under Medicare have had a significant effect on our revenue. The federal government and state governments continue to focus on efforts to curb spending on healthcare programs such as Medicare and Medicaid. We are not able to predict the outcome of the legislative process. We also cannot predict the extent to which proposals will be adopted or, if adopted and implemented, what effect, if any, such proposals and existing new legislation will have on us. Efforts to impose reduced allowances, greater discounts and more stringent cost controls by government and other payors are expected to continue and could adversely affect our business, financial condition and results of operations.
These include statutory and regulatory changes, rate adjustments (including retroactive adjustments), administrative or executive orders and government funding restrictions, all of which may materially adversely affect the rates at which Medicare reimburses us for our services. Budget pressures often lead the federal government to reduce or place limits on reimbursement rates under Medicare. Implementation of these and other types of measures has in the past, and could in the future, result in substantial reductions in our revenue and operating margins. For a discussion of historic adjustments and recent changes to the Medicare program and related reimbursement rates, see Part I, Item 1A Risk Factors under the headings Risks Related to Our Business and Industry.
22
Patient Protection and Affordable Care Act
Various healthcare reform provisions became law upon enactment of the Patient Protection and Affordable Care Act and the Healthcare Education and Reconciliation Act (collectively, the ACA). The reforms contained in the ACA have affected our operating subsidiaries in some manner and are directed in large part at increased quality and cost reductions. Several of the reforms are very significant and could ultimately change the nature of our services, the methods of payment for our services and the underlying regulatory environment. These reforms include modifications to the conditions of qualification for payment, bundling of payments to cover both acute and post-acute care and the imposition of enrollment limitations on new providers. The upcoming Congressional elections in the United States and policies implemented by the current and former Presidential administration have resulted in significant changes in legislation, regulation, implementation of Medicare, Medicaid and government policy. In August of 2022, Congress passed and the Biden-Harris Administration signed into law the Inflation Reduction Act of 2022 (IRA), which continued and expanded certain provisions of the ACA. Among other things, the IRA extended premium subsidies paid by the federal government, which were scheduled to expire at the end of 2022, until the end of 2024, resulting in subsidies being available to offset or reduce the costs of private health insurance policies for older persons on fixed incomes or with limited savings. This may aid older patients in obtaining or keeping their health insurance in order to pay for long-term care services. Other healthcare-related provisions of the IRA include phased-in provisions for Medicare to negotiate the prices of certain prescription drugs, limiting the out-of-pocket cost of prescribed drugs to Medicare Part D recipients to $2,000 per year (in addition to a monthly cap on out-of-pocket prescription drug expenses) and limiting the monthly cost of insulin to $35.
The outcomes of the 2022 midterm elections may significantly alter the current regulatory framework and impact our business and the health care industry, including any further extensions or expansions of certain ACA provisions, namely recent rulemaking activity regarding ACA Section 1557's anti-discrimination provisions. We continually monitor these developments so we can respond to the changing regulatory environment impacting our business.
Requirements of Participation
CMS has requirements that providers, including SNFs and other LTC facilities must meet in order to participate in the Medicare and Medicaid Programs. Some of these requirements can be burdensome and costly.
One such requirement of participation in the Medicare and Medicaid programs involves limitations around the use of pre-dispute, binding arbitration agreements by LTC facilities. CMS has issued guidance and direction around arbitration, to include: the facility must not require signing of an arbitration agreement as a condition of admission or a requirement to continue to receive care at the facility, and the agreement must expressly contain language to this effect; the facility must inform the resident or the resident's representative of the right not to sign the agreement; the facility must confirm that the agreement is explained in a manner that can be understood and that the resident or their representative acknowledges their understanding of the agreement; the agreement must provide for the right to rescind the agreement within 30 calendar days of signing; and the agreement may not contain language that prohibits or discourages communications with federal, state, or local officials, including federal and state surveyors, other federal or state health department employees, and representatives of the Office of the State Long-Term Care Ombudsperson. Congress has routinely introduced, but not passed, legislation addressing the issue of arbitration agreements used by LTC facilities. While legislative action is possible in the future, federal regulations and state/federal laws remain our primary source of authority over the use of pre-dispute binding arbitration agreements.
On June 29, 2022, CMS announced updated guidance for Phase 2 and 3 of the Requirements of Participation. CMS distributed these updates to surveyors and state agencies in order to, among other things, enhance responses to resident complaints and reported incidents. This updated guidance arises directly from President Biden’s March 2022 State of the Union Address and accompanying fact sheet regarding nursing home areas of study and potential change. The guidance focuses on the following topics: (1) resident abuse and neglect (including reporting of abuse); (2) admission, transfer and discharge; (3) mental health and substance abuse disorders; (4) nurse staffing and reporting of payroll to evaluate staffing sufficiency; (5) residents’ rights (including visitation); (6) potential inaccurate diagnoses or assessments; (7) prescription and use of pharmaceuticals, including psychotropics and drugs that act like psychotropics; (8) infection prevention and control; (9) arbitration of disputes between facilities and residents; (10) psychosocial outcomes and related severity; and (11) the timeliness and completion of state investigations to improve consistency in the application of standards among various states.
23
On July 29, 2022, CMS updated the Medicare Requirements of Participation for LTC facilities, which includes the modification of requirements associated with a facility's physical environment to minimize unnecessary renovation expenses that could result in the closure of LTC facilities because of the related expense. Specifically, CMS is "grandfathering" certain facilities and will allow LTC facilities that were participating in Medicare before July 5, 2016 and that previously used the Fire Safety Evaluation System (FSES) to continue using the 2001 FSES mandatory values when determining compliance with applicable standards. In addition, CMS updated the Requirements of Participation to include revising existing qualification requirements for directors of food and nutrition services in LTC facilities while "grandfathering" in directors with two or more years of experience and certain minimum training in food safety so that they may continue in that role without obtaining more specific educational and certification requirements.
In October of 2022, CMS published the survey resources CMS and state surveyors would be using to evaluate LTC facilities' compliance with vaccination and reporting requirements, which CMS updated in November of 2022. These updates provided more information for state surveyors to utilize when evaluating LTC facilities’ compliance with the Medicare Requirements of Participation, as well as included guidance for facilities on operationalizing compliance with these requirements based on how surveyors would measure and evaluate facility performance. On September 27, 2022, CMS also provided a summary of its major software enhancements, describing the tools updated and used by CMS to measure and evaluate LTC facility compliance with the Medicare Requirements of Participation.
Civil and Criminal Fraud and Abuse Laws and Enforcement
Various complex federal and state laws exist which govern a wide array of referrals, relationships and arrangements, and prohibit fraud by healthcare providers. Governmental agencies are devoting increasing attention and resources to such anti-fraud efforts. The Health Insurance Portability and Accountability Act of 1996 (HIPAA) and the Balanced Budget Act of 1997 expanded the penalties for healthcare fraud. Additionally, in connection with our involvement with federal healthcare reimbursement programs, the government or those acting on its behalf may bring an action under the FCA, alleging that a healthcare provider has defrauded the government by submitting a claim for items or services not rendered as claimed, which may include coding errors, billing for services not provided and submitting false or erroneous cost reports. The Fraud Enforcement and Recovery Act of 2009 (FERA) expanded the scope of the FCA by, among other things, creating liability for knowingly and improperly avoiding repayment of an overpayment received from the government and broadening protections for whistleblowers. The FCA clarifies that if an item or service is provided in violation of the AKS, the claim submitted for those items or services is a false claim that may be prosecuted under the FCA as a false claim. Civil monetary penalties under the FCA range from approximately $0.012 to $0.025 million per violation and are adjusted annually for inflation. Under the qui tam or “whistleblower” provisions of the FCA, a private individual with knowledge of fraud may bring a claim on behalf of the federal government and receive a percentage of the federal government’s recovery. Due to these whistleblower incentives, lawsuits have become more frequent. Many states also have a false claim prohibition that mirrors or closely tracks the federal FCA.
Federal law also provides that the OIG has the authority to exclude individuals and entities from federally funded health care programs on a number of grounds, including, but not limited to, certain types of criminal offenses, licensure revocations or suspensions and exclusion from state or other federal healthcare programs. CMS can recover overpayments from health care providers up to five years following the year in which payment was made. On February 28, 2022, the Administration published a fact sheet regarding nursing home care, which identified the Administration’s priorities of further funding for SNF and LTC facility inspections, enhancing civil penalties on poor-performing facilities and increasing the scrutiny of companies that operate more than one facility. Proposed rules based on these directives and studies are expected by early 2023, with final rules to follow after a notice-and-comment period.
In November 2019, the OIG released a report of its investigation into overpayments to hospitals that did not comply with Medicare’s post-acute-care transfer policy. Hospitals violating this policy transferred patients to certain post-acute-care settings, such as SNFs, but claimed the higher reimbursements associated with discharges to homes. A similar OIG audit report, released in February 2019, focused on improper payments for SNF services when the Medicare three-day inpatient hospital stay requirement was not met. In 2021, the OIG released the result of an audit finding that Medicare overpaid millions of dollars of chronic care management (CCM) services. The OIG's 2021 report found that in calendar years 2017 and 2018, Medicare overpaid millions of dollars in CCM claims. In 2022, the OIG released an audit revealing that CMS had not collected $226 million, or 45%, of identified overpayments within that period, potentially affecting SNFs. These investigatory actions by OIG demonstrate its increased scrutiny into post-hospital SNF care provided to beneficiaries and may encourage additional oversight or stricter compliance standards.
24
On numerous occasions, CMS has indicated its intent to vigilantly monitor overall payments to SNFs, paying particular attention to facilities that have high reimbursements for ultra-high therapy, therapy resource utilization groups with higher activities of daily living scores and long average lengths of stay. The OIG recognizes that there is a strong financial incentive for facilities to bill for higher levels of therapies, even when not needed by patients. We cannot predict the extent to which the OIG's recommendations to CMS will be implemented and, what effect, if any, such proposals would have on us. Our business model, like those of some other for-profit operators, is based in part on seeking out higher-acuity patients whom we believe are generally more profitable and over time our overall patient mix has consistently shifted to higher-acuity in most facilities we operate. We also use specialized care-delivery software that assists our caregivers in more accurately capturing and recording services in order to, among other things, increase reimbursement to levels appropriate for the care actually delivered. These efforts may place us under greater scrutiny with the OIG, CMS, our fiscal intermediaries, recovery audit contractors and others.
Federal Healthcare Reform
Five-Star Quality Reporting Metrics — The Quality Payment Program (QPP) was created under the Medicare Access and Children's Health Insurance Program (CHIP) Reauthorization Act of 2015. This program was based on the Merit-based Incentive Payment System (MIPS) or the use of Alternative Payment Models (APM), which relied on quality data CMS gathered and evaluated using the Five-Star Quality Rating system, which includes a rating of one to five in various categories. These categories include (but are not limited to) the results of surveys conducted by state inspectors, other health inspection outcomes, staffing, spending, readmissions and stay durations; the data collected and its weighting in determining a rating on a scale of one to five stars is subject to periodic and ongoing revision, re-balancing and adjustment by CMS to reflect market conditions and CMS’s priorities in patient care. Since 2020, CMS’s measurement of the data reported by providers, including SNFs, has become more competitive and resulted in a reduction of four- and five-star rankings available under CMS’s Five-Star Quality Rating system.
The Five-Star Quality reporting system for nursing homes is displayed on CMS's consumer-based Nursing Home Compare website. CMS also displays a consumer alert icon next to nursing homes that have been cited for incidents of abuse, neglect, or exploitation on the Nursing Home Compare website, which is updated monthly with CMS’s refresh of survey inspection results on that website.
In 2020, in response to the COVID-19 pandemic, CMS temporarily froze SNF Quality Reporting Program data, including data in the staffing and health inspection domains, on the Nursing Home Compare website to account for the then-suspended reporting and inspection obligations. After suspending inspections in early 2020, CMS announced a new and targeted inspection plan in August 2020 to focus on urgent patient safety threats and infection control, which affected the number of nursing homes inspected and the substance of those inspections. These safety inspections collected different information than traditional surveys and as a result these survey results were not incorporated in CMS’s Five-Star Quality ratings for SNFs from March through December 2020. CMS resumed calculating nursing homes’ health inspection ratings on January 27, 2021 and has continued to include this measure in subsequent updates.
Similarly, although staff reporting requirements were waived for the first six months of 2020, this waiver ended on June 25, 2020. Thereafter, SNFs were required to report staffing data to CMS, which was incorporated into CMS’s Five-Star Quality rating beginning in January 2021. The January 2021 Five-Star Quality rating calculation reflected SNF-provided quarterly updates of most quality measures for the period between June 2019 and June 2020, reflecting the time period in which the normal reporting and inspection obligations were frozen due to COVID-19. CMS’s refreshes of the Nursing Home Compare website since January of 2021 have included these quality measures and other new measures as discussed within this Government Regulation heading.
In January of 2022, CMS issued a bulletin stating that as of the same month, the Nursing Home Compare website would begin reporting SNF weekend staffing as well as staff tenure and other collected staffing data. Beginning in July of 2022, CMS began disclosing weekend staffing of all nurses, as well as staff turnover data for all nurses and administrators, on the Nursing Home Compare website. CMS also now incorporates this data into its Five-Star Quality ratings for SNFs and LTC facilities. This data is adjusted based on a facility's case mixture and evaluated on a quarterly basis. This data was included in the October 2022 refresh of the Nursing Home Care Compare website as well, in addition to increasing the thresholds for quality measures reported on the Nursing Home Care Compare website based on average improvement over prior quality measures.
25
Proposed Federal Legislation Concerning Nursing Home Supervision — On August 10, 2021, the Nursing Home Improvement and Accountability Act of 2021 (Nursing Home Improvement Act) was introduced in the U.S. Senate and was intended to update federal nursing home policy to improve quality of care and oversight. The proposed legislation would reduce SNF payments for inaccurate submission of certain data and provide federal funding to carry out SNF data validation and ensure accuracy of cost report information. The Nursing Home Improvement Act also proposed staffing requirements for SNFs and other measures intended to improve transparency, accountability and quality of care within nursing homes. If passed in its current form the bill would provide participating states with funds for up to six years in order to fund demonstrated improvements in nursing home workforce and care delivery. As of December 31, 2022, no action has been taken on this bill since its introduction to the Senate on August 10, 2021 and referral to the Senate Finance Committee that same day. A similar bill introduced in the United States House of Representatives in January of 2021 was introduced and referred to the Ways and Means Committee’s Healthcare Subcommittee on February 2, 2021.
Proposed State Legislation Concerning Nursing Home Supervision — California passed into law AB 35, which changes the limitations, or “caps,” on non-economic damages that can be awarded in medical negligence cases filed against healthcare providers (including skilled nursing and long-term care facilities). Beginning on January 1, 2023, non-economic damages (i.e. pain and suffering) available to plaintiffs suing healthcare providers in medical malpractice and professional negligence cases will be increased from $0.25 million to $0.35 million, and will then increase by $0.04 million per year over the following ten years up to a $0.75 million cap. Once the limit reaches $0.75 million, a 2% annual inflationary adjustment will attach beginning on January 1, 2034. In wrongful death cases that arise from claims of medical malpractice and professional negligence, the cap on non-economic damages will increase from $0.25 million to $0.50 million on January 1, 2023, and increase every year thereafter for ten years until the cap on non-economic damages in such cases is $1.0 million; thereafter, this cap will also be subject to an annual 2% increase to reflect changes in the cost of living. The caps are separate as to each claim, meaning that there is one cap for negligence and one cap for wrongful death. The new limits on non-economic damages apply prospectively to lawsuits filed on and after January 1, 2023.
On September 27, 2022, California’s Governor signed into law AB 1502, also known as the Skilled Nursing Facility Ownership and Management Reform Act of 2022. Expected to take effect on July 1, 2023, this law will affect new license applications for SNFs. AB 1502 increases the oversight authority of the California Department of Public Health, and changes several provisions regarding SNF licensing in the State of California. First, the law eliminates previous regulatory provisions that permitted SNFs to operate in advance of receiving their formal license from the State. AB 1502 also requires SNF license applicants to disclose additional information to the Department of Public Health in connection with a license application and requires the Department of Public Health to consider more data regarding the applicant’s prior operations before issuing it a license. This data includes, but is not limited to: prior citations; sanctions imposed by CMS; legal proceedings commenced by other State or Federal authorities; findings made regarding the applicant by agencies or courts; and actions taken against other facilities owned, operated, or managed by the applicant. The same analysis described above is intended to apply to applications for a change in ownership or a change in management of a skilled nursing facility. AB 1502 authorizes the Department of Public Health to impose civil penalties of up to $0.01 million, and other enforcement action as appropriate, upon applicants that fail to comply with the law’s requirements.
Proposed and Anticipated Administrative Action — On February 28, 2022, the Administration published a fact sheet stating its priorities for making changes to senior care, including potential changes to regulations affecting LTC and SNF facilities. The Administration’s priorities, which are to be studied throughout 2022, include transparency and public disclosure for nursing home owners and operators and an examination of the role of private equity investment, real estate investment trusts (REITs) and other investment interests in this sector. The SNF-VBP Program was also identified as an area for change, with staffing levels, retention and resident experience affecting reimbursement. Additional enforcement authority and resources, including enhanced scrutiny of poorly performing facilities and tools for improving their performance, is another Administration priority. The Administration also seeks to improve accessibility to nurse aide training, tie Medicaid payments to staff wages and benefits and enhance the recruitment and career paths for care workers. Finally, the Administration wishes to incorporate the lessons learned from the COVID-19 pandemic to impose new requirements for infection control, emergency preparedness and safety.
On April 11, 2022, CMS issued a proposed rule that could potentially lead to changes in the SNF-VBP Program, and setting SNF and LTC facility staffing levels. On June 29, 2022, CMS published guidance to surveyors for consistently evaluating Phase 2 and 3 Requirements of Participation for LTC facilities, addressing topics including infection control, resident safety, arbitration of disputes, nurse staffing and mental health disorders.
26
On September 22, 2022, CMS issued an IFR addressing nursing home visitation, including recommending the use of masks and face coverings to combat the transmission of COVID-19 and testing of symptomatic nursing home staff and residents regardless of COVID-19 vaccination status. On October 23, 2022, CMS issued further guidance unifying its recommendations for all facilities under its oversight, including SNFs and LTC facilities, reaffirming CMS's activities to verify COVID-19 vaccination of all SNF and LTC facility staff, and to pursue corrective action for facilities found deficient in this requirement.
Monitoring Compliance in Our Facilities
Governmental agencies and other authorities periodically inspect our independent operating facilities to assess compliance with various standards, rules and regulations. The robust regulatory and enforcement environment continues to impact healthcare providers, especially in connection with responses to any alleged noncompliance identified in periodic surveys and other inspections by governmental authorities. Unannounced surveys or inspections generally occur at least annually and may also follow a government agency's receipt of a complaint about a facility. Facilities must pass these inspections to maintain licensure under state law, to obtain or maintain certification under the Medicare and Medicaid programs, to continue participation in the Veterans Administration program at some facilities, and to comply with provider contracts with managed care clients at many facilities. From time to time, our independent operating subsidiaries, like others in the healthcare industry, may receive notices from federal and state regulatory agencies of an alleged failure to substantially comply with applicable standards, rules or regulations. These notices may require corrective action, may impose civil monetary penalties for noncompliance, and may threaten or impose other operating restrictions on SNFs such as admission holds, provisional skilled nursing license, or increased staffing requirements. If our independent operating subsidiaries fail to comply with these directives or otherwise fail to comply substantially with licensure and certification laws, rules and regulations, the facility could lose its certification as a Medicare or Medicaid provider, or lose its license permitting operation in the State.
Facilities with otherwise acceptable regulatory histories generally are normally given an opportunity to correct deficiencies and continue their participation in the Medicare and Medicaid programs by a certain date, usually within six months; however, although where denial of payment remedies are asserted, such interim remedies go into effect much sooner. Facilities with deficiencies that immediately jeopardize patient health and safety and those that are classified as poor performing facilities, however, may not be given an opportunity to correct their deficiencies prior to the imposition of remedies and other enforcement actions. Moreover, facilities with poor regulatory histories continue to be classified by CMS as poor performing facilities notwithstanding any intervening change in ownership, unless the new owner obtains a new Medicare provider agreement instead of assuming the facility's existing agreement. However, new owners nearly always assume the existing Medicare provider agreement due to the difficulty and time delays generally associated with obtaining new Medicare certifications, especially in previously certified locations with sub-par operating histories. Accordingly, facilities that have poor regulatory histories before acquisition by our independent operating subsidiaries and that develop new deficiencies after acquisition are more likely to have sanctions imposed upon them by CMS or state regulators.
In addition, CMS has increased its focus on facilities with a history of serious or sustained quality of care problems through the special focus facility (SFF) initiative. A facility's administrators and owners are notified when it is identified as a SFF. This information is also provided to the general public. Local state survey agencies recommend to CMS that facilities be placed on special focus status. SFFs receive heightened scrutiny and more frequent regulatory surveys. Failure to improve the quality of care can result in fines and termination from participation in Medicare and Medicaid. A facility “graduates” from the program once it demonstrates significant improvements in quality of care that are continued over a defined period of time.
On October 21, 2022, CMS issued a Memorandum identifying the changes it intends to make in connection with the oversight of those facilities that fall under the SFF Program. These proposed measures included increased penalties for SFFs that fail to improve their performance upon further inspection by CMS, increasing the standards SFFs must meet to graduate from the SFF program, maintaining heightened oversight of any SFF for a period of three years after it graduates and increasing the technical assistance CMS provides to SFFs. The CMS Memorandum also identifies grants that will be available to aid in the hiring, training and education of personnel involved in resident care, including licensed practical nurses and registered nurses. In addition to the communication from CMS, the White House also issued a fact sheet covering these same issues on October 21, 2022. The fact sheet further identified measures the Administration is taking to increase staffing requirements, halt illegal or improper debt collection activities, increase transparency in facility ownership and operation (including SNF performance), and tie reimbursement to the quality of performance.
27
Sanctions such as denial of payment for new admissions often are scheduled to go into effect before surveyors return to verify compliance. Generally, if the surveyors confirm that the facility is in compliance upon their return, the sanctions never take effect. However, if they determine that the facility is not in compliance, the denial of payment goes into effect retroactive to the date given in the original notice. This possibility sometimes leaves affected operators, including our independent subsidiaries, with the difficult task of deciding whether to continue accepting patients after the potential denial of payment date, thus risking the retroactive denial of revenue associated with those patients' care if the operators are later found to be out of compliance, or simply refusing admissions from the potential denial of payment date until the facility is actually found to be in compliance. In the past and from time to time, some of our independent operating subsidiaries have been or will be in denial of payment status due to findings of continued regulatory deficiencies, resulting in an actual loss of revenue associated with Medicare and Medicaid patients admitted after the denial of payment date. Additional sanctions could ensue and, if imposed, could include various remedies up to and including decertification.
CMS has undertaken several initiatives to increase or intensify Medicaid and Medicare survey and enforcement activities, including federal oversight of state actions. CMS is taking steps to focus more survey and enforcement efforts on facilities with findings of substandard care or repeat violations of Medicaid and Medicare standards and to identify multi-facility providers with patterns of noncompliance. CMS is also increasing its oversight of state survey agencies and requiring state agencies to use enforcement sanctions and remedies more promptly when substandard care or repeat violations are identified, to investigate complaints more promptly, and to survey facilities more consistently. On February 28, 2022, the Administration published a fact sheet regarding nursing home care, which identified the Administration’s priorities of further funding for SNF and LTC facility inspections, as well as enhanced penalties and other tools to use against non-compliant facilities. Proposed rules based on these directives and studies are expected in approximately one year, with final rules to follow a notice-and-comment period required by law.
Regulations Regarding Financial Arrangements
We are also subject to federal and state laws that regulate financial arrangement by and between healthcare providers, such as the federal and state anti-kickback laws, the Stark laws, and various state anti-referral laws.
The Social Security Act prohibits the knowing and willful offer, payment, solicitation, or receipt of any remuneration, directly or indirectly, overtly or covertly, in cash or in kind, to induce the referral of an individual, in return for recommending, or to arrange for, the referral of an individual for any item or service payable under any federal healthcare program, including Medicare or Medicaid. The OIG has issued regulations that create “safe harbors” for certain conduct and business relationships that are deemed protected under the Social Security Act. In order to receive safe harbor protection, all of the requirements of a safe harbor must be met. The fact that a given business arrangement does not fall within one of these safe harbors, however, does not render the arrangement per se illegal. Business arrangements of healthcare service providers that fail to satisfy the applicable safe harbor criteria, if investigated, will be evaluated based upon all facts and circumstances and risk increased scrutiny and possible sanctions by enforcement authorities.
Violations of the Social Security Act can result in inflation-adjusted criminal penalties of more than $0.1 million and ten years imprisonment. It can also result in inflation-adjusted civil monetary penalties of more than $0.1 million per violation and an assessment of up to three times the total amount of remuneration offered, paid, solicited, or received. It may also result in an individual's or organization's exclusion from future participation in federal healthcare programs. State Medicaid programs are required to enact an anti-kickback statute. Many states in which our independent operating subsidiaries operate have adopted or are considering similar legislative proposals, some of which extend beyond the Medicaid program, to prohibit the payment or receipt of remuneration for the referral of patients regardless of the source of payment for the care. We believe that business practices of providers and financial relationships between providers have become subject to increased scrutiny as healthcare reform efforts continue on the federal and state levels.
28
Additionally, the "Stark Law" of the Social Security Act provides that a physician may not refer a Medicare or Medicaid patient for a “designated health service” to an entity with which the physician or an immediate family member has a financial relationship unless the financial arrangement meets an exception under the Stark Law or its regulations. Designated health services include inpatient and outpatient hospital services, PT, OT, SLP, durable medical equipment, prosthetics, orthotics and supplies, diagnostic imaging, enteral and parenteral feeding and supplies and home health services. Under the Stark Law, a “financial relationship” is defined as an ownership or investment interest or a compensation arrangement. If such a financial relationship exists and does not meet a Stark Law exception, the entity is prohibited from submitting or claiming payment under the Medicare or Medicaid programs or from collecting from the patient or other payor. Many of the compensation arrangements exceptions permit referrals if, among other things, the arrangement is set forth in a written agreement signed by the parties, the compensation to be paid is set in advance, is consistent with fair market value and is not determined in a manner that takes into account the volume or value of any referrals or other business generated between the parties. Exceptions may have other requirements. Any funds collected for an item or service resulting from a referral that violates the Stark Law are not eligible for payment by federal healthcare programs and must be repaid to Medicare or Medicaid, any other third-party payor, and the patient. Violations of the Stark Law may result in the imposition of civil monetary penalties, including, treble damages. Individuals and organizations may also be excluded from participation in federal healthcare programs for Stark Law violations. Many states have enacted healthcare provider referral laws that go beyond physician self-referrals or apply to a greater range of services than just the designated health services under the Stark Law.
Regulations Regarding Patient Record Confidentiality
Health care providers are also subject to laws and regulations enacted to protect the confidentiality of patient health information. For example, HHS has issued rules pursuant to HIPAA, including the Health Information Technology for Economic and Clinical Health (HITECH) Act which governs our use and disclosure of protected health information of patients. We have established policies and procedures to comply with HIPAA privacy and security requirements at our independent operating subsidiaries. Our independent operating subsidiaries have adopted and implemented HIPAA compliance plans, which we believe comply with the HIPAA privacy and security regulations. The HIPAA privacy and security regulations have and will continue to impose significant costs on our independent operating subsidiaries in order to comply with these standards. There are numerous other laws and legislative and regulatory initiatives at the federal and state levels addressing privacy and security concerns. Our independent operating subsidiaries are also subject to any federal or state privacy-related laws that are more restrictive than the privacy regulations issued under HIPAA. These laws vary and could impose additional penalties for privacy and security breaches. Healthcare entities are also required to afford patients with certain rights of access to their health information under HIPAA and the 21st Century Cures Act (Cures Act). The Office of Civil Rights, the agency responsible for HIPAA enforcement, has targeted investigative and enforcement efforts on violations of patients’ rights of access, including denial of access to medical records, imposing significant fines for violations largely initiated from patient complaints. The Office of the National Coordinator for Health Information Technology can also investigate and impose separate penalties for information blocking violations under the Cures Act.
Antitrust Laws
We are also subject to federal and state antitrust laws. Enforcement of the antitrust laws against healthcare providers is common, and antitrust liability may arise in a wide variety of circumstances, including third party contracting, physician relations, joint venture, merger, affiliation and acquisition activities. In some respects, the application of federal and state antitrust laws to healthcare is still evolving, and enforcement activity by federal and state agencies appears to be increasing. At various times, healthcare providers and insurance and managed care organizations may be subject to an investigation by a governmental agency charged with the enforcement of antitrust laws, or may be subject to administrative or judicial action by a federal or state agency or a private party. Violators of the antitrust laws could be subject to criminal and civil enforcement by federal and state agencies, as well as by private litigants.
Americans with Disabilities Act
Our independent operating subsidiaries must also comply with the ADA, and similar state and local laws to the extent that the facilities are "public accommodations" as defined in those laws. The obligation to comply with the ADA and other similar laws is an ongoing obligation, and the independent operating subsidiaries continue to assess their facilities relative to ADA compliance and make appropriate modifications as needed.
29
Real Estate Investment Trust (REIT) Qualification
We are electing for Standard Bearer to be taxed as a REIT for U.S. federal income tax purposes beginning with its taxable year ended December 31, 2022. Standard Bearer's qualification as a REIT will depend upon its ability to meet, on a continuing basis, various complex requirements under the Internal Revenue Code, relating to, among other things, the sources of its gross income, the composition and value of its assets, distribution levels to its shareholders and the concentration of ownership of its capital stock. We believe that Standard Bearer is organized in conformity with the requirements for qualification and taxation as a REIT under the Code and that its manner of operation has and will enable it to continue to meet the requirements for qualification and taxation as a REIT.
REGULATIONS SPECIFIC TO SENIOR LIVING COMMUNITIES
As previously mentioned, senior living services revenue (approximately 2.2% of total revenue) is primarily derived from private pay residents, with a small portion of senior living revenue derived from Medicaid funds. Thus, some of the regulations discussed above applicable to Medicaid providers, also apply to senior living. However, the following provides a brief overview of the regulatory framework applicable specifically to senior living.
A majority of states provide, or are approved to provide, Medicaid payments for personal care and medical services to some residents in licensed senior living communities under waivers granted by or under Medicaid state plans approved by CMS. State Medicaid programs control costs for senior living and other home and community-based services by various means such as restrictive financial and functional eligibility standards, enrollment limits and waiting lists. Because rates paid to senior living community operators are generally lower than rates paid to SNF operators, some states use Medicaid funding of senior living services as a means of lowering the cost of services for residents who may not need the higher level of health services provided in SNFs. States that administer Medicaid programs for services in senior living communities are responsible for monitoring the services at, and physical conditions of, the participating communities. As a result of the growth of senior living in recent years, states have adopted licensing standards applicable to senior living communities. Most state licensing standards apply to senior living communities regardless of whether they accept Medicaid funding.
CMS has continued to commence a series of actions to increase its oversight of state quality assurance programs for senior living communities and has provided guidance and technical assistance to states to improve their ability to monitor and improve the quality of services paid through Medicaid waiver programs. CMS is encouraging state Medicaid programs to expand their use of home and community-based services as alternatives to facility-based services, pursuant to provisions of the ACA, and other authorities, through the use of several programs. As noted above, the Administration issued a fact sheet regarding nursing home care priorities and reforms that it intends to seek in the coming year. The Administration’s desired changes are multi-faceted, concerning payment to facilities, staffing level requirements, training and retention of staff, standards of care offered to residents, increased transparency and public disclosure of ownership, and enhanced civil remedies and other authority to exercise upon facilities that do not satisfy CMS’s standards. Proposed rules based on these directives are expected by early 2023, with final rules to follow a notice-and-comment period required by law. In 2022, CMS issued a proposed rule that requested information to be used for study and potential rulemaking consistent with the Administration’s February 28, 2022 fact sheet. CMS also published guidance to surveyors for consistently evaluating the requirements of participation for LTC facilities, specifically infection control, resident safety, arbitration of disputes, nurse staffing and mental health disorders.
The types of laws and statutes affecting the regulatory landscape of the post-acute industry continue to expand. In addition to this changing regulatory environment, federal, state and local officials are increasingly focusing their efforts on the enforcement of these laws. In order to operate our businesses, we must comply with federal, state and local laws relating to licensure, delivery and adequacy of medical care, distribution of pharmaceuticals, equipment, personnel, operating policies, fire prevention, rate-setting, billing and reimbursement, building codes and environmental protection. Additionally, we must also adhere to anti-kickback statues, physician referral laws, the ADA and safety and health standards set by the OSHA Administration. Changes in the law or new interpretations of existing laws may have an adverse impact on our methods and costs of doing business.
Our independent operating subsidiaries are also subject to various regulations and licensing requirements promulgated by state and local health and social service agencies and other regulatory authorities. Requirements vary from state to state and these requirements can affect, among other things, personnel education and training, patient and personnel records, services, staffing levels, monitoring of patient wellness, patient furnishings, housekeeping services, dietary requirements, emergency plans and procedures, certification and licensing of staff prior to beginning employment and patient rights. These laws and regulations could limit our ability to expand into new markets and to expand the services provided by independent operating subsidiaries in existing markets.
30
ENVIRONMENTAL MATTERS
We strive to reduce our environmental impact through initiatives to modernize our facilities, conserve water, optimize waste, work towards a paperless office and partner with green vendors. Our ongoing and planned facility modernization initiatives include solar projects, heating, ventilation and air condition (HVAC) upgrades, water systems updates, lighting retrofits and utility upgrades. Additionally, we track and evaluate the utilities used by our facilities to drive our initiatives. For the year ended December 31, 2022, we spent $87.5 million on purchases of property improvements and equipment which included facility modernization initiatives.
Our business is subject to a variety of federal, state and local environmental laws and regulations. As a healthcare provider, we face regulatory requirements in areas of air and water quality control, medical and low-level radioactive waste management and disposal, asbestos management, response to mold and lead-based paint in our facilities and employee safety.
As an owner or operator of our facilities, we also may be required to investigate and remediate hazardous substances that are located on and/or under the property, including any such substances that may have migrated off, or may have been discharged or transported from the property. Part of our operations involves the handling, use, storage, transportation, disposal and discharge of medical, biological, infectious, toxic, flammable and other hazardous materials, wastes, pollutants or contaminants. In addition, we are sometimes unable to determine with certainty whether prior uses of our facilities and properties or surrounding properties may have produced continuing environmental contamination or noncompliance, particularly where the timing or cost of making such determinations is not deemed cost-effective. These activities, as well as the possible presence of such materials in, on and under our properties, may result in damage to individuals, property or the environment; may interrupt operations or increase costs; may result in legal liability, damages, injunctions or fines; may result in investigations, administrative proceedings, penalties or other governmental agency actions; and may not be covered by insurance.
We believe that we are in material compliance with applicable environmental and occupational health and safety requirements. However, we cannot assure you that we will not encounter liabilities with respect to these regulations in the future, and such liabilities may result in material adverse consequences to our operations or financial condition.
AVAILABLE INFORMATION
We are subject to the reporting requirements under the Securities Exchange Act of 1934, as amended (the Exchange Act). Consequently, we are required to file reports and information with the Securities and Exchange Commission (SEC), including reports on the following forms: annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K, and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act. These reports, proxy and information statements and other information concerning our company may be accessed through the SEC's website at http://www.sec.gov.
You may also find on our website at www.ensigngroup.net, electronic copies of our annual reports on Form 10-K, quarterly reports on Form 10-Q, current reports on Form 8-K and amendments to those reports filed or furnished pursuant to Section 13(a) or 15(d) of the Exchange Act. Such filings are placed on our website as soon as reasonably possible after they are filed with the SEC. All such filings are available free of charge. The information contained in, or that can be accessed through, our website does not constitute a part of this Annual Report on Form 10-K.
31
Item 1A. RISK FACTORS
We are providing the following summary of the risk factors contained in our Form 10-K to enhance the readability and accessibility of our risk factor disclosures. We encourage our stockholders to carefully review the risk factors contained in this Form 10-K in their entirety for additional information regarding the risks and uncertainties that could cause our actual results to vary materially from recent results or from our anticipated future results.
Risks Related to our Business and Industry
•We face numerous risks related to the COVID-19 PHE and its expiration in 2023, which could individually or in the aggregate have a material adverse effect on our business, financial condition, liquidity, results of operations and prospects.
•Changes to reimbursement rates, rules and other aspects of Medicare and Medicaid, including reductions of the FMAP, could have a material, adverse effect on our revenues, financial condition and results of operations, including the reductions to reimbursement in the 2023 calendar year physician fee schedule and changes to data reporting, measurement and evaluation standards.
•Our revenue could be impacted by changes to existing reimbursement models.
•Reforms to the U.S. healthcare system, including new regulations under the ACA and its expansion under new laws such as the Inflation Reduction Act of 2022 (IRA) and future legislation, continue to impose new requirements upon us and may increase our costs or lower our reimbursements, which could materially impact our business.
•Changes to the U.S. healthcare system, including the Medicare program, may have unforeseen consequences for our business, including, but not limited to a loss of revenue, reduction of services covered by Medicare, limits on out-of-pocket expenses we may charge and other spending cuts that affect us in order to offset limitations on patient expenses for other medical services, such as the limitation on out-of-pocket expenses for prescription drugs.
•The recent midterm elections in 2022, may result in significant changes to the regulatory framework, enforcements, and reimbursements in our industry.
•We are subject to various government reviews, audits and investigations that could adversely affect our business, including an obligation to refund amounts previously paid to us, potential criminal charges, the imposition of fines, and/or the loss of our right to participate in Medicare and Medicaid programs.
•Public and government calls for increased survey and enforcement efforts toward LTC facilities, potential rulemaking that may result in enhanced enforcement and penalties, and new guidance for surveyors regarding the review of LTC facilities and enforcement of their Requirements of Participation, could result in increased scrutiny by state and federal survey agencies. Potential sanctions and remedies based upon alleged regulatory deficiencies could negatively affect our financial condition and results of operations.
•Future cost containment initiatives undertaken by third-party payors may limit our revenue and profitability.
•Changes in Medicare reimbursements for physician and non-physician services could impact reimbursement for medical professionals, which could have a negative effect on our business, financial condition or results of operations.
•We may be subject to increased investigation and enforcement activities related to HIPAA violations if we fail to adopt and maintain business procedures and systems designed to protect the privacy, security and integrity of patients’ individual health information.
•Security breaches and other cyber-security incidents could violate security laws and subject us to significant liability.
•If our independent operating subsidiaries are not fully reimbursed for all services for which each facility bills through consolidated billing, our revenue, financial condition and results of operations could be adversely affected.
•Increased competition for, or a shortage of, nurses and other skilled personnel could increase our staffing and labor costs and subject us to monetary fines resulting from a failure to maintain minimum staffing requirements, or may affect reimbursement.
•Annual caps and other cost-reductions for outpatient therapy services may reduce our future revenue and profitability or cause us to incur losses.
•Increased scrutiny of our billing practices by the Office of the Inspector General or other regulatory authorities may result in an increase in regulatory monitoring and oversight, decreased reimbursement rates, or otherwise adversely affect our business, financial condition and results of operations.
•State efforts to regulate or deregulate the healthcare services industry or the construction or expansion of healthcare facilities could impair our ability to expand our operations, or could result in increased competition.
•Newly enacted legislation in the States where our independently operating entities are located may impact the volume of cases filed and the overall cost of those cases from a defense and indemnity standpoint.
•Changes to federal and state employment-related laws and regulations could increase our cost of doing business.
•Required regulatory approvals could delay or prohibit transfers of our healthcare operations, which could result in periods in which we are unable to receive reimbursement for such properties.
•Compliance with federal and state fair housing, fire, safety, staffing, and other regulations may require us to incur unexpected expenses, which could be costly to us.
•We depend largely upon reimbursement from third-party payors, and our revenue, financial condition and results of operations could be negatively impacted by any changes in the acuity mix of patients in our affiliated facilities as well as payor mix and payment methodologies.
32
•We are subject to litigation that could result in significant legal costs and large settlement amounts or damage awards. Similarly, a change in the enforceability of arbitration provisions between LTC facilities and SNFs with residents or patients may affect the risks we face from claims and potential litigation.
•If our regular internal investigations into the care delivery, recordkeeping and billing processes of our operating subsidiaries detect instances of noncompliance, efforts to correct such non-compliance could materially decrease our revenue.
•We may be unable to complete future facility or business acquisitions at attractive prices or at all, or may elect to dispose of underperforming or non-strategic operating subsidiaries, either of which could decrease our revenue.
•We may not be able to successfully integrate acquired facilities and businesses into our operations, or we may be exposed to costs, liabilities and regulatory issues that may adversely affect our operations.
•If we do not achieve or maintain competitive quality of care ratings from CMS or private organizations engaged in similar monitoring activities, our business may be negatively affected.
•If we are unable to obtain insurance, or if insurance becomes more costly for us to obtain, our business may be adversely affected, and our self-insurance programs may expose us to significant and unexpected costs and losses.
•The geographic concentration of our affiliated facilities could leave us vulnerable to economic downturn, regulatory changes or acts of nature in those areas.
•The actions of a national labor union that has pursued a negative publicity campaign criticizing our business in the past may adversely affect our revenue and our profitability.
•The risks associated with leased property that our operators operate in could adversely affect our business, financial position or results of operations.
•Failure to generate sufficient cash flow to cover required payments or meet operating covenants under our long-term debt, mortgages and long-term operating leases could result in defaults under such agreements and cross-defaults under other debt, mortgage or operating lease arrangements, which could harm our operating subsidiaries and cause us to lose facilities or experience foreclosures.
•Move-in and occupancy rates may remain unpredictable even after the COVID-19 pandemic is over.
•A continued housing slowdown or housing downturn could decrease demand for senior living services.
•As we continue to acquire and lease real estate assets, we may not be successful in identifying and consummating these transactions.
•As we expand our presence in other relevant healthcare industries, we would become subject to risks in a market in which we have limited experience.
•If our referral sources fail to view us as an attractive skilled nursing provider, or if our referral sources otherwise refer fewer patients, our patient base may decrease.
•We may need additional capital to fund our operating subsidiaries and finance our growth, and we may not be able to obtain it on terms acceptable to us, or at all, which may limit our ability to grow.
•The condition of the financial markets, including recent and expected future increases to the federal funds rate, inflation and the consumer price index, could limit the availability of debt and equity financing sources to fund the capital and liquidity requirements of our business, as well as negatively impact or impair the value of our current portfolio of cash, cash equivalents and investments.
•Delays in reimbursement may cause liquidity problems.
•The continued use and growth of Medicaid managed care organizations may contribute to delays or reductions in our Medicaid reimbursement.
•Compliance with the regulations of the Department of Housing and Urban Development may require us to make unanticipated expenditures which could increase our costs.
•Failure to safeguard our patient trust funds may subject us to citations, fines and penalties.
•We are a holding company with no operations and rely upon our multiple independent operating subsidiaries to provide us with the funds necessary to meet our financial obligations. Liabilities of any one or more of our subsidiaries could be imposed upon us or our other subsidiaries.
•We may be exposed to liabilities as a result of the separation of Pennant, including if the spin-off is not tax-free for U.S. federal income tax purposes.
•Certain directors who serve on our Board of Directors also serve as directors of Pennant, and ownership of shares of Pennant common stock by our directors and executive officers may create, or appear to create, conflicts of interest.
•Standard Bearer's failure to qualify as a REIT may cause it to be subject to U.S. federal income tax. Additionally, legislative or other actions affecting REITs could have a negative effect on Standard Bearer.
Risks Related to Ownership of our Common Stock
•We may not be able to pay or maintain dividends and the failure to do so would adversely affect our stock price.
•Our amended and restated certificate of incorporation, amended and restated bylaws and Delaware law contain provisions that could discourage transactions resulting in a change in control, which may negatively affect the market price of our common stock.
33
You should carefully consider each of the following risk factors and all other information set forth in this information statement. The risk factors generally have been separated into two categories: risks relating to our business and our industry and risks relating to our common stock. Based on the information currently known to us, we believe that the following information identifies the most significant risk factors affecting our company in each of these categories of risks. However, the risks and uncertainties we face are not limited to those set forth in the risk factors described below. Additional risks and uncertainties not presently known to us or that we currently believe to be immaterial may also adversely affect our business. In addition, past financial performance may not be a reliable indicator of future performance and historical trends should not be used to anticipate results or trends in future periods.
If any of the following risks and uncertainties develops into actual events, these events could have a material adverse effect on our business, financial condition or results of operations. In such case, the trading price of our common stock could decline. You should carefully read the following risk factors, together with the financial statements, related notes and other information contained in this Annual Report on Form 10-K. This Annual Report on Form 10-K contains forward-looking statements that contain risks and uncertainties. Please refer to the section entitled "Cautionary Note Regarding Forward-Looking Statements" on page 1 of this Annual Report on Form 10-K in connection with your consideration of the risk factors and other important factors that may affect future results described below.
Risks Related to Our Business and Industry
We face numerous risks related to the COVID-19 PHE, which could have a material adverse effect on our business, financial condition, liquidity, results of operations and prospects.
The extent to which the COVID-19 PHE will continue impacting our operations will depend on future developments, which are highly uncertain and cannot be predicted with confidence, including future waves of COVID-19 variants and their severity, ongoing federal and state vaccination programs and requirements and the efficacy of vaccinations and the ongoing actions to contain the virus or treat its impact, among others. Some of the risks of COVID-19 are being mitigated as a result of the federal vaccination program, including vaccinations and vaccine booster requirements of nursing facility staff and residents, but there remains uncertainty as to what changes will be made to HHS’s emergency response to reflect the evolving and endemic nature of COVID-19, analogous to seasonal spikes in influenza cases and the final details for unwinding the PHE's Emergency Waivers and other administrative flexibilities at the federal and state levels.
As discussed in Item 1., under Government Regulation, federal, state and local regulators have implemented new regulations and waived existing regulations to promote care delivery during the COVID-19 PHE. While the majority of these changes are beneficial by reducing regulatory burdens, these accommodations may also have an adverse effect through increased legal and operational costs related to compliance and monitoring. Additionally, most of the accommodations are limited in duration and tied to the PHE declaration, thus there may be significant operational change requirements on short notice. As of December 31, 2022, sixteen of the Emergency Waivers relevant to SNFs and LTC facilities expired. Also, the reinstatement of waived state and federal regulations may not occur simultaneously, requiring heightened monitoring to ensure compliance.
Other factors from the continuation of the COVID-19 pandemic that could have an adverse effect on our business, financial condition, liquidity, results of operations and prospects, include:
•potential for permanent government regulations and restrictions to combat COVID-19;
•increased strain on employees and resources caused by different waves of COVID-19 variants with different infection and effects, affecting employee availability and capacity to work;
•reduced occupancy as a result of concerns of residents and their families related to COVID-19 transmissibility within LTC settings, as well as due to government-imposed orders;
•increased costs related to additional and changing CDC protocols, federal and state workforce protection and related isolation procedures, including obligations to test patients and staff for COVID-19 vaccination mandates;
•limitations on availability of staff due to COVID-19 related illness or exposure, or due to unwillingness to comply with vaccine mandates;
•increased scrutiny by regulators of infection control and prevention measures, including increased reporting requirements related to suspected and confirmed COVID-19 diagnoses of residents and staff, which may result in fines or other sanctions related to non-compliance;
•increased risk of litigation and related liabilities arising in connection with patient or staff illness, hospitalization and/or death;
34
•negative impacts on our patients' ability or willingness to pay for healthcare services and our third parties' ability or willingness to pay rents; and
•regulations that require all of our workers to be fully vaccinated, including receiving vaccination boosters, against COVID-19 as a condition of participating in the Medicare and Medicaid programs.
•complexity, uncertainty and potential state-by-state rulemaking arising from the expiration of the COVID-19 PHE and expiration of Emergency Waivers.
The extent and duration of the impact of the COVID-19 pandemic on our stock price is uncertain, our stock price may be more volatile, and our ability to raise capital could be impaired.
Our revenue could be impacted by federal and state changes to reimbursement and other aspects of Medicare.
We derived 27.7% and 27.8% of our service revenue from the Medicare programs for the years ended December 31, 2022 and 2021, respectively. In addition, many other payors may use published Medicare rates as a basis for reimbursements. Accordingly, if Medicare reimbursement rates are reduced or fail to increase as quickly as our costs, if there are changes in the rules governing the Medicare program that are disadvantageous to our business or industry, or if there are delays in Medicare payments, our business and results of operations will be adversely affected.
The Medicare program and its reimbursement rates and rules are subject to frequent change. These include statutory and regulatory changes, rate adjustments (including retroactive adjustments), annual caps that limit the amount that can be paid (including deductible and coinsurance amounts) administrative or executive orders and government funding restrictions, all of which may materially adversely affect the rates at which Medicare reimburses us for our services. Budget pressures often lead the federal government to reduce or place limits on reimbursement rates under Medicare. Implementation of these and other types of measures has in the past and could in the future result in substantial reductions in our revenue and operating margins. For example, see Item 1., under Government Regulation, Sequestration of Medicare Rates.
Additionally, Medicare payments can be delayed or declined due to determinations that certain costs are not reimbursable or reasonable because either adequate or additional documentation was not provided or because certain services were not covered or considered medically necessary. Additionally, revenue from these payors can be retroactively adjusted after a new examination during the claims settlement process or as a result of post-payment audits. New legislation and regulatory proposals could impose further limitations on government payments to healthcare providers.
In addition, CMS often changes the rules governing the Medicare program, including those governing reimbursement. Changes to the Medicare program that could adversely affect our business include:
•administrative or legislative changes to base rates or the bases of payment;
•limits on the services or types of providers for which Medicare will provide reimbursement;
•changes in methodology for patient assessment and/or determination of payment levels;
•changes in staff requirements (i.e., requiring all workers to be vaccinated against COVID-19 and receive booster injections for those vaccinations) as a condition of payment or eligibility for Medicare reimbursement (See also, Item 1., under Government Regulation);
•the reduction or elimination of annual rate increases, or the end of the reduced payments deferment (See also, Item 1., under Government Regulation); or
•an increase in co-payments or deductibles payable by beneficiaries.
Among the important statutory changes that are being implemented by CMS are provisions of the IMPACT Act. This law imposes a stringent timeline for implementing benchmark quality measures and data metrics across post-acute care providers (long stay hospitals, inpatient rehabilitation facilities, skilled nursing facilities (SNFs), and home health agencies). The enactment also mandates specific actions to design a unified payment methodology for post-acute providers. CMS continues to promulgate regulations to implement provisions of this enactment. Depending on the final details, the costs of implementation could be significant. The failure to meet implementation requirements could expose providers to fines and payment reductions.
35
Reductions in reimbursement rates or the scope of services being reimbursed could have a material, adverse effect on our revenue, financial condition and results of operations or even result in reimbursement rates that are insufficient to cover our operating costs. Loss of Medicare reimbursement entirely would also have a material adverse effect on our revenue. Medicare may rescind our certification and terminate its payor agreements if not all of our employees are fully vaccinated consistent with CMS's IFR requiring vaccination of SNF employees, which has applied to all states since March 21, 2022. In addition, within certain states such as California and Washington, if our employees are not fully vaccinated as required by those states’ vaccination mandates, we could incur a deficiency that could endanger our Medicaid certification and participation status for certain locations within those states where employees have not been vaccinated. In addition, California required employees to receive at least one booster dose of the COVID-19 vaccine by March 1, 2022 in order to comply with its State Public Health Officer Order requiring vaccination of SNF employees. Other states where we operate, such as Colorado, have allowed their COVID-19 vaccinations to expire, or did not impose such mandates for the state’s healthcare workers. Any penalty, suspension, termination, or other sanction under any state’s Medicaid program could lead to reciprocal and commensurate penalties being imposed under the Medicare program, up to termination or rescission of our Medicare participation and payor agreements as noted above. Additionally, any delay or default by the government in making Medicare reimbursement payments could materially and adversely affect our business, financial condition and results of operations.
Reductions in Medicaid reimbursement rates or changes in the rules governing the Medicaid program could have a material, adverse effect on our revenue, financial condition and results of operations.
A significant portion of reimbursement for skilled nursing services comes from Medicaid. In fact, Medicaid is our largest source of revenue, accounting for 46.0% and 45.8% of our revenue for the years ended December 31, 2022 and 2021, respectively. Medicaid is a state-administered program financed by both state funds and matching federal funds. Medicaid spending has increased rapidly in recent years, becoming a significant component of state budgets, which has led both the federal government and many states to institute measures aimed at controlling the growth of Medicaid spending, and in some instances reducing aggregate Medicaid spending. Since a significant portion of our revenue is generated from our skilled nursing operating subsidiaries in California, Texas and Arizona, any budget reductions or delays in these states could adversely affect our net patient service revenue and profitability. Despite present state budget surpluses in many of the states in which we operate, we can expect continuing cost containment pressures on Medicaid outlays for SNFs, and any such decline could adversely affect our financial condition and results of operations.
The Medicaid program and its reimbursement rates and rules are subject to frequent change at both the federal and state level. These include statutory and regulatory changes, rate adjustments (including retroactive adjustments), administrative or executive orders and government funding restrictions, all of which may materially adversely affect the rates at which our services are reimbursed by state Medicaid plans. To generate funds to pay for the increasing costs of the Medicaid program, many states utilize financial arrangements commonly referred to as provider taxes. Under provider tax arrangements, states collect taxes from healthcare providers and then use the revenue to pay the providers as a Medicaid expenditure, which allows the states to then claim additional federal matching funds on the additional reimbursements. Current federal law provides for a cap on the maximum allowable provider tax as a percentage of the providers' total revenue. There can be no assurance that federal law will continue to provide matching federal funds on state Medicaid expenditures funded through provider taxes, or that the current caps on provider taxes will not be reduced. Any discontinuance or reduction in federal matching of provider tax-related Medicaid expenditures could have a significant and adverse effect on states' Medicaid expenditures, and as a result could have a material and adverse effect on our business, financial condition or results of operations.
Upcoming changes to Medicaid reimbursement and FMAP may affect our revenues.
The bipartisan omnibus spending plan passed by Congress and signed into law by the President on December 29, 2022, contains provisions that will wind down and end increased FMAP payments provided for by FFCRA, as well as provide for the disenrollment of Medicaid beneficiaries who have participated in the program since early in the COVID-19 pandemic. In the first quarter of 2023, the FMAP increase CMS provides to the States will remain elevated by 6.2%, but will decline for the remaining quarters in 2023, at 5% in the second quarter, 2.5% in the third quarter, and 1.5% in the fourth quarter before increased FMAP spending ends entirely. Previously, the FMAP funding was dependent on the termination of the PHE. The ultimate amount of funding from each state will vary substantially based on that states’ policies. This may result in reductions in Medicaid spending by states where we operate, causing reductions in rates, and delays or withholding of payment for our operating subsidiaries’ services and effect our operating subsidiaries’ ability to profitably perform their services.
36
CMS’s ability to further reduce these declining amounts of increased FMAP payments to states may create further pressure on Medicaid reimbursement in states where we operate. The omnibus spending plan also grants CMS the authority to impose fines, penalties, and other sanctions upon states that do not comply with this law’s requirements for the unwinding of increased FMAP payments. As a result, these reductions may impose further burdens on the Medicaid programs in states where we operate, which may result in reduced payments.
Additionally, beginning on April 1, 2023, states may begin disenrolling Medicaid beneficiaries. CMS guidance regarding disenrollment of beneficiaries and a return to historical renewal, enrollment, and eligibility determination practices permits states up to 14 months to initiate and process traditional Medicaid renewals, including the eligibility and enrollment process. The allowance of disenrollment and return to traditional Medicaid renewal processes, which will include pre-COVID eligibility determinations, may result in a reduction of the number of Medicaid beneficiaries and may result in a reduction of our current and potential patient population. As a result, there may be fewer current or potential patients able to pay for our operating subsidiaries’ services, and increased competition for Medicaid beneficiaries able to provide reimbursement for those services.
Our revenue could be impacted by changes to existing reimbursement models.
As discussed in more detail in Item 1., under Government Regulation, CMS implemented a final rule in October 2019 to replace the existing case-mix classification system, Resource Utilization Groups, Version IV, with a new case-mix classification system, PDPM, that focuses more on the clinical condition of the patient and less on the volume of services provided. CMS may make future adjustments to reimbursement levels as it continues to monitor the impact of PDPM on patient outcomes and budget neutrality. CMS could remove the entire parity calculated adjustment and this would cause a drastic reduction in payments. In addition, the Administration continues to study the nursing home industry and for HHS to issue proposed rules based on those studies, including changes to SNF-VBP Program, may also adversely affect our reimbursement. The Administration continues to act on the issues identified in its February 28, 2022 fact sheet and further regulation is expected regarding LTC and SNF reimbursement. CMS elected to defer the SNF 30-Day All-Cause Readmission Measure (SNFRM) as part of performance scoring for fiscal year 2023, although the SNFRM will still be reported without affecting SNF payment. This final rule also provided for the SNF-VBP program expansion beyond the use of its single, all-cause hospital readmission measure to determine payment, with the inclusion of measures beginning in fiscal year 2026 for SNF healthcare associated infections requiring hospitalization (SNF HAI) and total nursing hours per resident day measures. Beginning in fiscal year 2027, the SNF-VBP program will also consider the discharge to community - post acute care measure for SNFs, which assesses the rate of successful discharges to the community from a SNF setting.
Reforms to the U.S. healthcare system continue to impose new requirements upon us and may increase our costs or lower our reimbursements.
The ACA included sweeping changes to how healthcare is paid for and furnished in the U.S. Applicable to our business, as discussed in greater detail in Item 1., under Government Regulation, the ACA has resulted in significant changes to our operations and reimbursement models for services we provide. CMS continues to issue rules to implement the ACA, including most recently new rules regarding the implementation of the anti-discrimination provisions. Courts continue to interpret and apply the ACA’s provisions. With the passage of the IRA in August of 2022, Congress continues to expand and supplement the ACA, including through the continuation of federally funded insurance premium subsidies for health insurance coverage purchased on the ACA-created marketplace for individual health insurance. This modification of the ACA by the IRA indicates that Congress may continue to change and expand the ACA in the future.
The efficacy of the ACA is the subject of much debate among members of Congress and the public. Additionally, a number of lawsuits have been filed challenging various aspects of the ACA and related regulations with inconsistent outcomes - some expand the ACA while others limit the ACA. In the event that the ACA is repealed or materially amended as a result of future challenges, particularly any elements of the ACA that are beneficial to our business or that cause changes in the health insurance industry, including reimbursement and coverage by private, Medicare or Medicaid payers, our business, operating results and financial condition could be harmed. Thus, the future impact of the ACA on our business is difficult to predict and its continued uncertain future may negatively impact our business. However, any material changes to the ACA or its implementing regulations may negatively impact our operations.
37
Similarly, the proposed Nursing Home Improvement Act may have an impact on our business due to the proposed two percent decrease in payments to SNFs, as well as the staffing and reporting requirements contained within the bill. This bill primarily creates penalties such as reduced reimbursement and monetary penalties for submitting inaccurate cost reports or staffing data. If passed in its current form, however, this bill would provide participating states with a temporary enhanced federal Medicaid match to fund improvements in nursing home workforce and care. This match would last six years, and states would be responsible for showing CMS that Medicaid reimbursement increases were used to increase worker wages and yield new training resources and opportunities for nursing home staff. While it is difficult to determine whether the Nursing Home Improvement Act will be amended prior to adoption, or even passed into law, if passed, this bill may negatively impact our business, with the scope and nature of its consequences unknown. As of December 31, 2022, however, the Nursing Home Improvement Act has not advanced out of the committee where it was introduced, and the same is true for a companion bill introduced in the House of Representatives.
Statements that the Administration made earlier this year indicate that HHS and CMS are being instructed to study the nursing home industry, specifically with regard to staffing levels, and the Administration has called for greater oversight of LTC and SNF facilities—including greater penalties for non-compliance with federal laws and regulations. On April 11, 2022, CMS issued a proposed rule that requested information to be used for study and potential rulemaking. Based upon this information-gathering and subsequent study, HHS and CMS are expected to issue new rules that may subject our business to greater oversight, increase penalties that the Government may seek to impose upon us, and impose additional conditions and measurements upon the reimbursement we receive from Medicare and Medicaid. In addition, CMS has published guidance to surveyors for consistently evaluating requirements of participation for LTC facilities, addressing topics including infection control, resident safety, arbitration of disputes, nurse staffing and mental health disorders. Surveyors' use of these additional Requirements of Participation to evaluate our affiliated facilities may increase our costs of compliance and subject us to additional fines and penalties for alleged non-compliance. CMS has also requested additional information from the public and industry participants that is expected to be used by HHS and CMS in creating additional regulations regarding staffing and operations of SNFs and LTC facilities in the future. These anticipated regulations, consistent with the Administration’s prior statements, may adversely affect our business, its operations, and its profitability.
We cannot predict what effect future reforms to the U.S. healthcare system will have on our business, including the demand for our services or the amount of reimbursement available for those services. However, it is possible these new laws may lower reimbursement or increase the cost of doing business and adversely affect our business.
The results of recent U.S. midterm elections in 2022 may result in significant changes to regulatory framework, enforcements and reimbursements.
The most recent midterm elections in 2022 could result in significant changes in, and uncertainty with respect to, legislation, regulation, implementation or repeal of laws and rules related to government health programs, including Medicare and Medicaid. Democratic proposals for Medicare for All or significant expansion of Medicare, could significantly impact our business and the healthcare industry if implemented. Additionally, Congress’s passage of the IRA in August of 2022, which expanded upon and continued certain provisions of the ACA through administrative rule-making, indicates that additional legislative changes to the ACA may be forthcoming based on the limited changes in the political composition of the House of Representatives and Senate following the November 2022 mid-term elections. If proposed policies specific to nursing facilities are implemented, these may result in significant regulatory changes, increased survey frequency and scope, and increased penalties for non-compliance.
We continually monitor these developments in order to respond to the changing regulatory environment impacting our business. While it is not possible to predict whether and when any such changes will occur, specific proposals discussed during and after the election, including a repeal or material amendment of the ACA (whether to increase or decrease its scope), could harm our business, operating results and financial condition. If we are slow or unable to adapt to any such changes, our business, operating results and financial condition could be adversely affected.
Our business may be materially impacted if certain aspects of the ACA are amended, repealed, or successfully challenged.
A number of lawsuits have been filed challenging various aspects of the ACA and related regulations. In addition, the ACA may be affected by both the recently completed midterm elections and forthcoming Presidential and Congressional elections in 2024. Cases challenging the ACA or related rules have had inconsistent outcomes - some expand the ACA while others limit the ACA. Thus, the future impact of the ACA on our business is difficult to predict. The uncertainty as to the future of the ACA may negatively impact our business, as will any material changes to the ACA.
38
In the event that legal challenges are successful or the ACA is repealed or materially amended, particularly any elements of the ACA that are beneficial to our business or that cause changes in the health insurance industry, including reimbursement and coverage by private, Medicare or Medicaid payers, our business, operating results and financial condition could be harmed. While it is not possible to predict whether and when any such changes will occur, specific proposals discussed during and after the election, including a repeal or material amendment of the ACA, could harm our business, operating results and financial condition. In addition, even if the ACA is not amended or repealed, the President and the executive branch of the federal government, as well as CMS and HHS have a significant impact on the implementation of the provisions of the ACA, and a new administration could make changes impacting the implementation and enforcement of the ACA, which could harm our business, operating results and financial condition. If we are slow or unable to adapt to any such changes, our business, operating results and financial condition could be adversely affected.
We are subject to various government reviews, audits and investigations that could adversely affect our business, including an obligation to refund amounts previously paid to us, potential criminal charges, the imposition of fines, and/or the loss of our right to participate in Medicare and Medicaid programs.
As a result of our participation in the Medicaid and Medicare programs, we are subject to various governmental reviews, audits and investigations to verify our compliance with the rules associated with these programs and related applicable laws and regulations. We are subject to regulatory reviews relating to Medicare services, billings and potential overpayments resulting from the actions of Recovery Audit Contractors, Zone Program Integrity Contractors, Program Safeguard Contractors, Unified Program Integrity Contractors, Supplemental Medical Review Contractors and Medicaid Integrity Contractors programs, (collectively referred to as Reviews), in which third party firms engaged by CMS conduct extensive reviews of claims data and medical and other records to identify potential improper payments under the Federal and State programs. As discussed above, the Administration has called for HHS and CMS to increase the level of scrutiny in these audits and has requested those agencies to adopt rules that would impose greater penalties upon non-compliant LTC and SNF operators.
On June 29, 2022, CMS announced updated guidance for Phase 2 and 3 of the requirements of participation. The guidance updates the following topics: (1) resident abuse and neglect (including reporting of abuse); (2) admission, transfer and discharge; (3) mental health and substance abuse disorders; (4) nurse staffing and reporting of payroll to evaluate staffing sufficiency; (5) residents’ rights (including visitation); (6) potential inaccurate diagnoses or assessments; (7) prescription and use of pharmaceuticals, including psychotropics and drugs that act like psychotropics; (8) infection prevention and control; (9) arbitration of disputes between facilities and residents; (10) psychosocial outcomes and related severity; and (11) the timeliness and completion of state investigations to improve consistency in the application of standards among various states. The application of CMS’s new guidance could result in more aggressive and stringent surveys, and potential fines, penalties, sanctions, or administrative actions taken against our independent operating subsidiaries.
Private pay sources also reserve the right to conduct audits. We believe that billing and reimbursement errors and disagreements are common in our industry. We are regularly engaged in reviews, audits and appeals of our claims for reimbursement due to the subjectivities inherent in the process related to patient diagnosis and care, record keeping, claims processing and other aspects of the patient service and reimbursement processes, and the errors and disagreements those subjectivities can produce. An adverse review, audit or investigation could result in:
•an obligation to refund amounts previously paid to us pursuant to the Medicare or Medicaid programs or from private payors, in amounts that could be material to our business;
•state or federal agencies imposing fines, penalties or other sanctions on us;
•temporary or permanent loss of our right to participate in the Medicare or Medicaid programs or one or more private payor networks;
•an increase in private litigation against us; and
•damage to our reputation in the geographies served by our independent operating subsidiaries.
Medicare administrative contractors conduct selected reviews of claims previously submitted by and paid to some of our independent operating entities. Although we have always been subject to post-payment audits and reviews, more intensive “probe reviews” performed in recent years appear to be a regular procedure with our fiscal intermediaries. All findings of overpayment from CMS contractors are eligible for appeal through the CMS defined processes and procedures. With the exception of rare findings of overpayment related to objective errors in Medicare payment methodology or claims processing, we utilize all defenses reasonably available to us to demonstrate that the services provided meet all clinical and regulatory requirements for reimbursement.
39
In cases where claim and documentation review by any CMS contractor results in repeated unsatisfactory results, an operation can be subjected to protracted regulatory oversight. This oversight may include repeat education and re-probe, extended pre-payment review, referral to recovery audit or integrity contractors, or extrapolation of an error rate to other reimbursement outside of specifically reviewed claims. Sustained failure to demonstrate improvement towards meeting all claim filing and documentation requirements could ultimately lead to Medicare decertification. As of December 31, 2022 and since, 34 of our independent operating subsidiaries had reviews scheduled, on appeal, or in a dispute resolution process, either pre- or post-payment. We anticipate that these reviews could increase in frequency in the future.
Additionally, both federal and state government agencies have heightened and coordinated civil and criminal enforcement efforts as part of numerous ongoing investigations of healthcare companies and, in particular, SNFs. The focus of these investigations includes, among other things:
•cost reporting and billing practices;
•quality of care;
•financial relationships with referral sources; and
•medical necessity of services provided.
On May 31, 2018, we received a Civil Investigative Demand (CID) from the DOJ stating that it is investigating our company to determine whether we have violated the FCA or the Anti-Kickback Statute with respect to the relationships between certain of our SNFs and persons who served as medical directors, advisory board participants or other referral sources. The CID covered the period from October 3, 2013 through 2018 and was limited in scope to ten of our Southern California SNFs. In October 2018, the Department of Justice made an additional request for information covering the period of January 1, 2011 through 2018, relating to the same topic. As a general matter, our operating entities maintain policies and procedures to promote compliance with the FCA, the Anti-Kickback Statute, and other applicable regulatory requirements. We are fully cooperating with the U.S. Department of Justice. In April 2020, the Company was advised that the U.S. Department of Justice declined to intervene in any subsequent action filed by a relator in connection with the subject matter of this investigation.
If we should agree to a settlement of, claims or obligations under federal Medicare statutes, the federal FCA, or similar State and Federal statutes and related regulations, our business, financial condition and results of operations and cash flows could be materially and adversely affected, and our stock price could be adversely impacted. Among other things, any settlement or litigation could involve the payment of substantial sums to settle any alleged civil violations and may also include our assumption of specific procedural and financial obligations going forward under a corporate integrity agreement or other arrangement with the government.
If the government or a court were to conclude that errors and deficiencies constitute criminal violations and/or that such errors and deficiencies resulted in the submission of false claims to federal healthcare programs, or were to discover other problems in addition to the ones identified by the probe reviews that rose to actionable levels, we and certain of our officers might face potential criminal charges and civil claims, administrative sanctions and penalties for amounts that could be material to our business, results of operations and financial condition. In addition, we or some of the key personnel of our independent operating subsidiaries could be temporarily or permanently excluded from future participation in state and federal healthcare reimbursement programs such as Medicaid and Medicare.
If any of our independently operated subsidiary facilities is decertified or loses its licenses, our revenue, financial condition or results of operations would be adversely affected. In addition, the report of such issues at any of our independently operated subsidiary facilities could harm our reputation for quality care and lead to a reduction in the patient referrals to and ultimately a reduction in occupancy at these facilities. Also, responding to auditing and enforcement efforts diverts material time, resources and attention away from our management team and our staff, and could have a materially detrimental impact on our results of operations during and after any such investigation or proceedings, regardless of whether we prevail on the underlying claim.
We are subject to extensive and complex laws and government regulations. If we are not operating in compliance with these laws and regulations or if these laws and regulations change, we could be required to make significant expenditures or change our operations in order to bring our facilities and operations into compliance.
We, along with other companies in the healthcare industry, are required to comply with extensive and complex laws and regulations at the federal, state and local government levels relating to, among other things:
40
•licensure and certification;
•adequacy and quality of healthcare services;
•qualifications and vaccination (including boosting) of healthcare and support personnel;
•quality of medical equipment;
•confidentiality, maintenance and security issues associated with medical records and claims processing;
•relationships with physicians and other referral sources and recipients;
•constraints on protective contractual provisions with patients and third-party payors;
•operating policies and procedures;
•addition of facilities and services; and
•billing for services.
The laws and regulations governing our operations, along with the terms of participation in various government programs, regulate how we do business, the services we offer, and our interactions with patients and other healthcare providers. These laws and regulations are subject to frequent change. As noted above, the Administration has called upon HHS and CMS to study and propose new rules regarding staffing requirements and reimbursement for the nursing home industry, including tying reimbursement to staffing levels, salary, benefits, and retention. CMS's guideline and sanction addressed topics including infection control, resident safety, arbitration of disputes, nurse staffing, and mental health disorders. In addition, CMS' new guidance including the use of masks and face coverings in connection with visitations to combat the transmission of COVID-19, testing of nursing home staff and residents regardless of COVID-19 vaccination status and verifying vaccination of all SNF and LTC facility staff could result in enhanced scrutiny by state surveyors and a potential increase in fines, penalties, sanctions, or administrative actions against our independent operating subsidiaries.
We believe that such regulations may increase in the future and we cannot predict the ultimate content, timing or impact on us of any healthcare reform legislation. Changes in existing laws or regulations, or the enactment of new laws or regulations, could negatively impact our business. If we fail to comply with these applicable laws and regulations, we could suffer civil or criminal penalties and other detrimental consequences, including denial of reimbursement, imposition of fines, temporary suspension of admission of new patients, suspension or decertification from the Medicaid and Medicare programs, restrictions on our ability to acquire new facilities or expand or operate existing facilities, the loss of our licenses to operate and the loss of our ability to participate in federal and state reimbursement programs. Additionally, in the future, different interpretations or enforcement of these laws and regulations could subject our current or past practices to allegations of impropriety or illegality or could require us to make changes in our facilities, equipment, personnel, services, capital expenditure programs and operating expenses.
As discussed in greater detail in Item 1., under Government Regulation, we are subject to federal and state laws intended to prevent healthcare fraud and abuse, including the federal FCA, state false claims acts, the illegal remuneration provisions of the Social Security Act, the AKS, state anti-kickback laws, the Civil Monetary Penalties Law and the federal “Stark” Law. Among other things, these laws prohibit kickbacks, bribes and rebates, as well as other direct and indirect payments or fee-splitting arrangements that are designed to induce the referral of patients to a particular provider for medical products or services payable by any federal healthcare program and prohibit presenting a false or misleading claim for payment under a federal or state program. They also prohibit some physician self-referrals. Possible sanctions for violation of any of these restrictions or prohibitions include loss of eligibility to participate in federal and state reimbursement programs and civil and criminal penalties. If we fail to comply, even inadvertently, with any of these requirements, we could be required to alter our operations, refund payments to the government, enter into a corporate integrity agreement, deferred prosecution or similar agreements with state or federal government agencies, and become subject to significant civil and criminal penalties.
These anti-fraud and abuse laws and regulations are complex, and we do not always have the benefit of significant regulatory or judicial interpretation of these laws and regulations. While we do not believe we are in violation of these prohibitions, we cannot assure you that governmental officials charged with the responsibility for enforcing these prohibitions will not assert that we are violating the provisions of such laws and regulations. Our company is currently aware of an investigation by the DOJ related to allegations some of our California facilities may have violated the FCA or the AKS with respect to the relationships between certain of our SNFs and persons who served as medical directors, advisory board participants or other referral sources. While our operating entities maintain policies and procedures to promote compliance with the FCA, the AKS, and other applicable regulatory requirements, we cannot predict when the investigation will be resolved, the outcome of the investigation or its potential impact on our company.
41
We are unable to predict the future course of federal, state and local regulation or legislation, including Medicare and Medicaid statutes and regulations related to fraud and abuse, the intensity of federal and state enforcement actions or the extent and size of any potential sanctions, fines or penalties. Changes in the regulatory framework, our failure to obtain or renew required regulatory approvals or licenses or to comply with applicable regulatory requirements, the suspension or revocation of our licenses or our disqualification from participation in federal and state reimbursement programs, or the imposition of other enforcement sanctions, fines or penalties could have a material adverse effect upon our business, financial condition or results of operations. Furthermore, should we lose licenses or certifications for a number of our facilities or other businesses as a result of regulatory action or legal proceedings, we could be deemed to be in default under some of our agreements, including agreements governing outstanding indebtedness.
Public and government calls for increased survey and enforcement efforts toward LTC facilities, and potential rulemaking that may result in enhanced enforcement and penalties, could result in increased scrutiny by state and federal survey agencies. In addition, potential sanctions and remedies based upon alleged regulatory deficiencies could negatively affect our financial condition and results of operations.
As CMS turns its attention to enhancing enforcement activities towards LTC facilities, as discussed in Item 1., under Government Regulation, state survey agencies will have more accountability for their survey and enforcement efforts. The Administration’s fact sheet regarding enhanced penalties against SFFs, discussed in greater length within that section, represents further federal calls for oversight and penalties for low-ranked and underperforming LTC facilities. This fact sheet precedes greater focus by CMS in obtaining oversight over SFFs, and continuing that oversight even after those SFFs improve, and subjecting them to more exacting and routine oversight. The likely result may be more frequent surveys of our affiliated facilities, with more substantial penalties, fines and consequences if they do not perform well. For low-performing facilities in the SFF program, the standards for successfully emerging from that program and not being subject to ongoing and enhanced government oversight will be higher and measured over a longer period of time, prolonging the risks of monetary penalties, fines and potential suspension or exclusion from the Medicare and Medicaid programs.
As discussed in Item 1., under Government Regulation, from time to time in the ordinary course of business, we receive deficiency reports from state and federal regulatory bodies resulting from such inspections or surveys. The focus of these deficiency reports tends to vary from year to year and state to state. Based on its October 2022 guidance, CMS and its state surveyors will place greater emphasis on COVID-19 vaccination reporting and will potentially assess penalties for failing to comply with vaccination administration and reporting obligations. Although most inspection deficiencies are resolved through an agreed-upon plan of corrective action, the reviewing agency typically has the authority to take further action against a licensed or certified facility, which could result in the imposition of fines, imposition of a license to a conditional or provisional status, suspension or revocation of a license, suspension or denial of payment for new admissions, loss of certification as a provider under state or federal healthcare programs, or imposition of other sanctions, including criminal penalties. In the past, we have experienced inspection deficiencies that have resulted in the imposition of a provisional license and could experience these results in the future.
Furthermore, in some states, citation of one affiliated facility could negatively impact other affiliated facilities in the same state. Revocation of a license at a given facility could therefore impair our ability to obtain new licenses or to renew, or maintain, existing licenses at other facilities, which may also trigger defaults or cross-defaults under our leases and our credit arrangements, or adversely affect our ability to operate or obtain financing in the future. If state or federal regulators were to determine, formally or otherwise, that one facility's regulatory history ought to impact another of our existing or prospective facilities, this could also increase costs, result in increased scrutiny by state and federal survey agencies, and even impact our expansion plans. Therefore, our failure to comply with applicable legal and regulatory requirements in any single facility could negatively impact our financial condition and overall of operations results.
From time to time, we have opted to voluntarily stop accepting new patients pending completion of a new state survey, in order to avoid possible denial of payment for new admissions during the deficiency cure period, or simply to avoid straining staff and other resources while retraining staff, upgrading operating systems or making other operational improvements. If we elect to voluntary close any operations in the future or to opt to stop accepting new patients pending completion of a state or federal survey, it could negatively impact our financial condition and results of operation.
We have received notices of potential sanctions and remedies based upon alleged regulatory deficiencies from time to time, and such sanctions have been imposed on some of our affiliated facilities. We have had affiliated facilities placed on special focus facility status in the past, continue to have some facilities on this status currently and other operating subsidiaries may be identified for such status in the future. We currently have no facilities placed on special focus facility status.
42
Future cost containment initiatives undertaken by private third-party payors may limit our revenue and profitability.
Our non-Medicare and non-Medicaid revenue and profitability are affected by continuing efforts of third-party payors to maintain or reduce costs of healthcare by lowering payment rates, narrowing the scope of covered services, increasing case management review of services and negotiating pricing. In addition, sustained unfavorable economic conditions may affect the number of patients enrolled in managed care programs and the profitability of managed care companies, which could result in reduced payment rates. There can be no assurance that third party payors will make timely payments for our services, or that we will continue to maintain our current payor or revenue mix. Trade publications within the healthcare industry have reported on the trend of payors using the No Surprises Act as a means to force re-negotiation of reimbursement rates for providers and facilities, and this trend has led to ongoing litigation between these providers and/or facilities against payors. Although the services provided in our business generally are outside the scope of the No Surprises Act, subsequent rulemaking and potentially aggressive behaviors by payors may pose a risk to our business. We are continuing our efforts to develop our non-Medicare and non-Medicaid sources of revenue and any changes in payment levels from current or future third-party payors could have a material adverse effect on our business and consolidated financial condition, results of operations and cash flows.
Changes in Medicare reimbursements for physician and non-physician services could impact reimbursement for medical professionals.
As discussed in greater detail in Item 1., under Government Regulation, MACRA revised the payment system for physician and non-physician services. Section 1 of that law, the sustainable growth rate repeal and Medicare Provider Payment Modernization will impact payment provisions for medical professional services. That enactment also extended for two years provisions that permit an exceptions process from therapy caps imposed on Medicare Part B outpatient therapy. There was a combined cap for PT and SLP and a separate cap for OT services that apply subject to certain exceptions. On February 9, 2018, the BBA was signed into law, which provides for the repeal of all therapy caps retroactively to January 1, 2018. The law also reduced the monetary threshold that triggers a manual medical review (MMR), in certain instances through 2028. The reduction in the MMR threshold will likely result in increased number of reviews for the foreseeable future, which could in turn have a negative effect on our business, financial condition or results of operations.
We may be subject to increased investigation and enforcement activities related to HIPAA violations.
We are required to comply with numerous legislative and regulatory requirements at the federal and state levels addressing patient privacy and security of health information, as discussed in greater detail in Item 1., under Government Regulation. HIPAA, as amended by the HITECH Act, requires us to adopt and maintain business procedures and systems designed to protect the privacy, security and integrity of patients' individual health information. States also have laws that apply to the privacy of healthcare information. We must comply with these state privacy laws to the extent that they are more protective of healthcare information or provide additional protections not afforded by HIPAA. If we fail to comply with these state and federal laws, we could be subject to criminal penalties, civil sanctions, litigation, and be forced to modify our policies and procedures. Additionally, if a breach under HIPAA or other privacy laws were to occur, remediation efforts could be costly and damage to our reputation could occur.
In addition to breaches of protected patient information, under HIPAA and the 21st Century Cures Act (Cures Act), healthcare entities are also required to afford patients with certain rights of access to their health information. Recently, the Office of Civil Rights, the agency responsible for HIPAA enforcement, has targeted investigative and enforcement efforts on violations of patients’ rights of access, imposing significant fines for violations largely initiated from patient complaints. If we fail to comply with our obligations under HIPAA, we could face significant fines. Likewise, if we fail to comply with our obligations under the Cures Act, we could face fines from the Office of the National Coordinator for Health Information Technology, the agency responsible for Cures Act enforcement.
43
Security breaches and other cyber-security incidents could violate security laws and subject us to significant liability.
Healthcare businesses are increasingly the target of cyberattacks whereby hackers disrupt business operations or obtain protected health information, often demanding large ransoms. In 2021 alone, the healthcare sector saw a 45% increase in ransomware attacks, with the average cost to remediate being over $1 million per incident. Our business is dependent on the proper functioning and availability of our computer systems and networks. While we have taken steps to protect the safety and security of our information systems and the patient health information and other data maintained within those systems, we cannot assure you that our safety and security measures and disaster recovery plan will prevent damage, interruption or breach of our information systems and operations. Additionally, we cannot control the safety and security of our information held by third-party vendors with whom we contract. Because the techniques used to obtain unauthorized access, disable or degrade service, or sabotage systems change frequently and may be difficult to detect, we (or third-party vendors) may be unable to anticipate these techniques or implement adequate preventive measures. In addition, hardware, software or applications we (or third-party vendors) develop or procure from third parties may contain defects in design or manufacture or other problems that could unexpectedly compromise the security of information systems. Unauthorized parties may attempt to gain access to our systems or facilities, or those of third parties with whom we do business, through fraud or other forms of deceiving our employees or contractors.
On occasion, we have acquired additional information systems through our business acquisitions, and these acquired systems may expose us to risk. We also license certain third-party software to support our operations and information systems. Our inability, or the inability of third-party vendors, to continue to maintain and upgrade information systems and software could disrupt or reduce the efficiency of our operations. In addition, costs and potential problems and interruptions associated with the implementation of new or upgraded systems and technology or with maintenance or adequate support of existing systems also could disrupt or reduce the efficiency of our operations.
A cyber-attack or other incident that bypasses our information systems security could cause a security breach which may lead to a material disruption to our information systems infrastructure or business, significant costs to remediate (e.g., payment to cyber attackers to recover our data) and may involve a significant loss of business or patient health information. If a cyber-attack or other unauthorized attempt to access our systems or facilities were to be successful, it could result in the theft, destruction, loss, misappropriation or release of confidential information or intellectual property, and could cause operational or business delays that may materially impact our ability to provide various healthcare services. Any successful cyber-attack or other unauthorized attempt to access our systems or facilities also could result in negative publicity which could damage our reputation or brand with our patients, referral sources, payors or other third parties and could subject us to a number of adverse consequences, the vast majority of which are not insurable, including but not limited to significant payment to cyber attackers to recover data, disruptions in our operations, regulatory and other civil and criminal penalties, fines, investigations and enforcement actions (including, but not limited to, those arising from the SEC, Federal Trade Commission, Office of Civil Rights, the OIG or state attorneys general), fines, private litigation with those affected by the data breach, loss of customers, disputes with payors and increased operating expense, which either individually or in the aggregate could have a material adverse effect on our business, financial position, results of operations and liquidity.
We may not be fully reimbursed for all services for which each facility bills through consolidated billing, which could adversely affect our revenue, financial condition and results of operations.
SNFs are required to perform consolidated billing for certain items and services furnished to patients and residents. The consolidated billing requirement essentially confers on the SNF itself the Medicare billing responsibility for the entire package of care that its patients receive in these situations. The BBA also affected SNF payments by requiring that post-hospitalization skilled nursing services be “bundled” into the hospital's diagnostic related group (DRG) payment in certain circumstances. Where this rule applies, the hospital and the SNF must, in effect, divide the payment which otherwise would have been paid to the hospital alone for the patient's treatment, and no additional funds are paid by Medicare for skilled nursing care of the patient. Although this provision applies to a limited number of DRGs, it has a negative effect on SNF utilization and payments, either because hospitals are finding it difficult to place patients in SNFs which will not be paid as before or because hospitals are reluctant to discharge the patients to SNFs and lose part of their payment. This bundling requirement could be extended to more DRGs in the future, which would accentuate the negative impact on SNF utilization and payments. We may not be fully reimbursed for all services for which each facility bills through consolidated billing, which could adversely affect our revenue, financial condition and results of operations.
44
Increased competition for, or a shortage of, nurses and other skilled personnel could increase our staffing and labor costs and subject us to monetary fines.
Our success depends upon our ability to retain and attract nurses and other skilled personnel, such as Certified Nurse Assistants, social workers and speech, physical and occupational therapists. Our success also depends upon our ability to retain and attract skilled management personnel who are responsible for the day-to-day operations of each of our affiliated facilities. Each facility has a facility leader responsible for the overall day-to-day operations of the facility, including quality of care, social services and financial performance. Depending upon the size of the facility, each facility leader is supported by facility staff that is directly responsible for day-to-day care of the patients and marketing and community outreach programs. Other key positions supporting each facility may include individuals responsible for physical, occupational and speech therapy, food service and maintenance. We compete with various healthcare service providers, including other skilled nursing providers, in retaining and attracting qualified and skilled personnel.
We operate one or more affiliated SNFs in the states of Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin. With the exception of Utah, which follows federal regulations, each of these states has established minimum staffing requirements for facilities operating in that state. Failure to comply with these requirements can, among other things, jeopardize a facility's compliance with the conditions of participation under relevant state and federal healthcare programs. In addition, if a facility is determined to be out of compliance with these requirements, it may be subject to a notice of deficiency, a citation, or a significant fine or litigation risk. Deficiencies (depending on the level) may also result in the suspension of patient admissions and the termination of Medicaid participation, or the suspension, revocation or non-renewal of the SNF's license. If the federal or state governments were to issue regulations which materially change the way compliance with the minimum staffing standard is calculated or enforced, our labor costs could increase and the current shortage of healthcare workers could impact us more significantly, including the increased scrutiny on staffing at the state and federal levels as a result of the COVID-19 virus. The broader labor market where we compete is in a unique state of disequilibrium where the needs of businesses such as ours outstrip the supply of available and willing workers. There is additional upward pressure on wages from different industries and more generally due to the reported rate of inflation for the preceding 12 months. Some of these industries compete with us for labor and others that do not, which makes it difficult to make significant hourly wage and salary increases due to the fixed nature of our reimbursement under insurance contracts as well as Medicare and Medicaid, in addition to our increasing variable costs. Due to the limited supply of qualified applicants who seek or are willing to accept employment, these broader concerns, as well as those specific to both federal COVID-19 vaccination mandates and existing state mandates, may increase our labor costs or lead to potential staffing shortages, reduced operations to comply with applicable laws and regulations, or difficulty complying with those laws and regulations at current operational levels.
Federal laws and regulations may increase our costs of maintaining qualified nursing and skilled personnel, or make it more difficult for us to attract or retain qualified nurses and skilled staff members. The proposed Nursing Home Improvement Act, if passed into law in substantially the same form as the proposed bill, may increase our responsibility to provide nursing coverage and the costs associated with that increased coverage. There has been an increase in the Administration's desire to have HHS and CMS study staffing level requirements for the nursing home industry and to tie Medicare and Medicaid reimbursement to the salary, benefits, and retention of staff. CMS has published guidance to surveyors addressing topics that specifically include nurse staffing and collection of payroll data to evaluate appropriate staffing levels, requiring the use of masks and face coverings by staff and testing of nursing home staff and residents regardless of COVID-19 vaccination status, emphasizing the scope of information to be gathered from and reported by facilities, including SNFs and LTC facilities and emphasizing the penalties for non-compliance, as well as the obligations of facilities seeking to demonstrate their corrective actions. These requirements may also increase our operating costs and require additional compensation to be paid to employees in the form of wages and benefits. We are monitoring our facilities for potential effects from CMS's IFR requiring employees of Medicare and Medicaid-participating medical facilities to be vaccinated, which may cause disruption to our affiliated facilities’ nursing staff and may additionally disrupt our operations if affected personnel decline to be vaccinated and replacement staffing cannot be located.
45
Similar state-level requirements in the states where our affiliated SNFs operate, whether such requirements are passed by statute, regulation, or executive order, may result in a shortage or inability to obtain nurses and skilled staff. As noted above, California, Washington, and Colorado have all mandated vaccinations for workers in health care facilities that include nursing homes. These administrative mandates precede, may be more restrictive than and are not likely to be preempted by CMS's IFR. As of July 14, 2022, however, Colorado’s Board of Health allowed its emergency rule requiring all healthcare workers be vaccinated against COVID-19 to expire, other than those working within Medicare and Medicaid-certified facilities. At this time, state vaccine mandates, including their status and enforcement, continues to be an area that varies widely from state to state, and as seen by Colorado permitting its mandate to expire, is subject to ongoing change. While federal litigation over the COVID-19 vaccination IFR has concluded, federal enforcement of this IFR remains an enforcement priority and could subject our affiliated SNFs to scrutiny and potential fines, penalties, and other consequences for non-compliance up to and including suspension or termination of their authorization to operate. State survey authorities that are tasked with enforcing their own state’s mandate have similar powers to screen for compliance and impose fines and penalties for non-compliance, including suspension or termination of operating licenses.
Increased competition for, or a shortage of, nurses or other trained personnel, or general ongoing inflationary pressures may require that we enhance our pay and benefits packages to compete effectively for such personnel. We may not be able to offset such added costs by increasing the rates we charge to the patients of our operating subsidiaries. Turnover rates and the magnitude of the shortage of nurses or other trained personnel vary substantially from facility to facility. An increase in costs associated with, or a shortage of, skilled nurses, could negatively impact our business. In addition, if we fail to attract and retain qualified and skilled personnel, our ability to conduct our business operations effectively could be harmed. Additionally, turnover in nursing staff, particularly among registered nurses, may adversely affect us and the ratings of the facilities we operate under the new five-star measurement formulation used by the Nursing Home Compare website, when quality measure thresholds were increased, making it more difficult for our affiliated SNFs to obtain the highest scores.
Annual caps and other cost-reductions for outpatient therapy services may reduce our future revenue and profitability or cause us to incur losses.
As discussed in detail in Item 1., under Government Regulation, sub-heading Part B Rehabilitation Requirements, several government actions have been taken in recent years to try and contain the costs of rehabilitation therapy services provided under Medicare Part B, including the MPPR, institution of annual caps, mandatory medical reviews for annual claims beyond a certain monetary threshold, and a reduction in reimbursement rates for therapy assistant claim modifiers. Of specific concern has been CMS's decision to lower Medicare Part B reimbursement rates for outpatient therapy services by 9%, beginning on January 1, 2021. These reductions continued in 2022 and are expected to continue in 2023 pursuant to the 2023 PFS final rule. Such cost-containment measures and ongoing payment changes could have an adverse effect on our revenue.
The Office of the Inspector General or other regulatory authorities may choose to more closely scrutinize billing practices in areas where we operate or propose to expand, which could result in an increase in regulatory monitoring and oversight, decreased reimbursement rates, or otherwise adversely affect our business, financial condition and results of operations.
As discussed in greater detail in Item 1., under Government Regulation, Civil and Criminal Fraud and Abuse Laws and Enforcement, the OIG regularly conducts investigations regarding certain payment or compliance issues within various healthcare sectors. Following these investigations, the OIG publishes reports, in part, to educate involved stakeholders and signal future enforcement focus. Reports published in 2019 and 2020 demonstrate the OIG’s increased scrutiny on post-hospital SNF care and continues to identify SNF compliance as an issue in its 2021 and 2022 semi-annual reports to Congress. This may impact the SNF industry by motivating additional reviews and stricter compliance in the areas outlined in the recent reports, expending material time and resources. Recent publications and statements by the Administration have also called for greater scrutiny of SNF and LTC facilities based on OIG's 2022 findings that these facilities did not implement appropriate infection control measures during the COVID-19 pandemic, and calling for more authorities to impose penalties and other remedies on facilities that violate federal laws and regulations.
46
Additionally, OIG reports published in 2010 and 2015 show the OIG’s concerns related to the billing practices of SNFs based on Medicare Part A claims and financial incentives for facilities to bill for higher levels of therapies, even when not needed by patients. In its fiscal year 2014 work plan, and again in 2017, OIG specifically stated that it will continue to study and report on questionable Part A and Part B billing practices amongst SNFs. Recently, in its 2021 work plan, OIG stated it will evaluate whether payments to SNFs under PDPM complied with Medicare requirements. OIG’s 2022 work plan states it will use a series of audits to confirm compliance with COVID-19 vaccination requirements for LTC facility staff and will study nursing home emergency preparedness—particularly with managing resident care and collaborating with other health care providers. The study findings of nursing home emergency preparedness will be used to develop a key performance indicator to track challenges faced by nursing homes over time. On May 19, 2022, the OIG updated its Nursing Homes webpage, stating its key goals for nursing home oversight were (1) to protect residents from fraud, abuse and neglect, and to promote quality of resident care; (2) promote emergency preparedness and response efforts; and (3) to strengthen frontline oversight. Each of these priorities could signal an increased focus on compliance with the Requirements of Participation and other laws and regulations applicable to SNF and LTC facilities. OIG last updated its website regarding nursing homes in November of 2022, noting that an additional purpose of OIG’s mission was to support the federal monitoring of nursing homes to mitigate risks to residents.
Our business model, like those of some other for-profit operators, is based in part on seeking out higher-acuity patients whom we believe are generally more profitable, and over time our overall patient mix has consistently shifted to higher-acuity and higher-resource utilization patients in most facilities we operate. We also use specialized care-delivery software that assists our caregivers in more accurately capturing and recording activities of daily living services, among other things. These efforts may place us under greater scrutiny with the OIG, CMS, our fiscal intermediaries, recovery audit contractors and others.
State efforts to regulate or deregulate the healthcare services industry or the construction or expansion of healthcare facilities could impair our ability to expand our operations, or could result in increased competition.
Some states require healthcare providers, including SNFs, to obtain prior approval, known as a certificate of need, for: (i) the purchase, construction or expansion of healthcare facilities; (ii) capital expenditures exceeding a prescribed amount; or (iii) changes in services or bed capacity.
In addition, other states that do not require certificates of need have effectively barred the expansion of existing facilities and the establishment of new ones by placing partial or complete moratoria on the number of new Medicaid beds they will certify in certain areas or in the entire state. Other states have established such stringent development standards and approval procedures for constructing new healthcare facilities that the construction of new facilities, or the expansion or renovation of existing facilities, may become cost-prohibitive or extremely time-consuming. In addition, some states require the approval of the state Attorney General for acquisition of a facility being operated by a non-profit organization.
Our ability to acquire or construct new facilities or expand or provide new services at existing facilities would be adversely affected if we are unable to obtain the necessary approvals, if there are changes in the standards applicable to those approvals, or if we experience delays and increased expenses associated with obtaining those approvals. We may not be able to obtain licensure, certificate of need approval, Medicaid certification, state Attorney General approval or other necessary approvals for future expansion projects. Conversely, the elimination or reduction of state regulations that limit the construction, expansion or renovation of new or existing facilities could result in increased competition to us or result in overbuilding of facilities in some of our markets. If overbuilding in the skilled nursing industry in the markets in which we operate were to occur, it could reduce the occupancy rates of existing facilities and, in some cases, might reduce the private rates that we charge for our services.
Newly enacted legislation in the States where our independently operating entities are located may impact the volume of cases filed and the overall cost of those cases from a defense and indemnity standpoint.
For example, AB 35 in the State of California was recently signed into law, which increases the cap of non-economic damages awarded to plaintiffs who are successful in medical malpractice litigation. The cap increases from $0.25 million to $0.35 million beginning on January 1, 2023, with incremental increases over the following 10 years until the cap reaches a maximum of $0.75 million. In wrongful death cases, the cap increases from $0.25 million to $0.5 million on January 1, 2023, with incremental increases over the following 10 years until the cap reaches a maximum of $1 million. Due to the influence of California on other states, other jurisdictions where we operate may enact similar laws and increase their current limits on damages in medical malpractice litigation depending on the outcomes of upcoming elections.
47
Additionally, California’s adoption of AB 1502, discussed in Item 1., Government Regulation, imposes new requirements for obtaining licenses to operate SNFs. These new requirements may delay the ability to obtain new SNF licenses within that state, whether through acquisition of existing facilities or opening a new facility. The additional background research that California’s Department of Public Health is required to engage in may increase the costs of obtaining licensure, make applications more time-consuming and complex, and may result in civil penalties and other sanctions against our affiliated facilities in the event they are not compliant with these new licensure application requirements. As a result, this new law may delay or impede growth within California. As with AB 35, California’s influence on other states may result in this legislation becoming a model for other states and having similar, potentially adverse effects within those jurisdictions as well.
Changes to federal and state employment-related laws and regulations could increase our cost of doing business.
Our operating subsidiaries are subject to a variety of federal and state employment-related laws and regulations, including, but not limited to, the U.S. Fair Labor Standards Act which governs such matters as minimum wages, overtime and other working conditions, the ADA and similar state laws that provide civil rights protections to individuals with disabilities in the context of employment, public accommodations and other areas, the National Labor Relations Act, regulations of the EEOC, regulations of the Office of Civil Rights, regulations of state attorney generals, family leave mandates and a variety of similar laws enacted by the federal and state governments that govern these and other employment law matters.
On November 17, 2022, a coalition of 22 states formally called on the Biden-Harris administration to withdraw its vaccine mandate for healthcare workers and all related guidance. Other than this petition, the uncertain environment regarding COVID-19 vaccination mandates and potential attempts to enforce similar mandates in 2022 appear to have concluded and there is no nationally significant litigation concerning such mandates. Nonetheless, the possibility of future or related action regarding COVID-19 vaccination mandates is one we are monitoring, as it represents a risk of uncertainty to the Company that may result in limitations on staff availability, disruption caused by staff departure, potential claims under the ADA and other laws and potential government sanctions which could cause disruptions to the operations of our subsidiaries, limit our ability to grow and otherwise adversely affect our business and financial results. Furthermore, the Administration has requested HHS and CMS study and issue proposed rules regarding the sustainability of care-based careers, including improving access to training, increasing the attractiveness of compensation in care-based positions, and improving the retention and career progression of care workers. The Administration has sought proposed rules that tie some of these issues, such as wages and retention, to Medicare reimbursement for facilities. Rising operating costs due to labor shortages, greater compensation and incentives required to attract and retain qualified personnel and higher-than-usual inflation on items including energy, utilities, food and other goods used in our facilities and the costs for transporting these items could increase our cost and decrease our profits.
The compliance costs associated with these laws and evolving regulations could be substantial. For example, all of our affiliated facilities are required to comply with the ADA. The ADA has separate compliance requirements for “public accommodations” and “commercial properties,” but generally requires that buildings be made accessible to people with disabilities. Compliance with ADA requirements could require removal of access barriers and non-compliance could result in imposition of government fines or an award of damages to private litigants. Further legislation may impose additional burdens or restrictions with respect to access by disabled persons. In addition, federal proposals to introduce a system of mandated health insurance and flexible work time and other similar initiatives could, if implemented, adversely affect our operations. We also may be subject to employee-related claims such as wrongful discharge, discrimination or violation of equal employment law. While we are insured for these types of claims, we could be subject to damages that are not covered by our insurance policies or that exceed our insurance limits, and we may be required to pay such damages directly, which would negatively impact our cash flow from operations.
Required regulatory approvals could delay or prohibit transfers of our healthcare operations, which could result in periods in which we are unable to receive reimbursement for such properties.
The operations of our operating subsidiaries must be licensed under applicable state law and, depending upon the type of operation, certified or approved as providers under the Medicare and/or Medicaid programs. In the process of acquiring or transferring operating assets, our operations must receive change of ownership approvals from state licensing agencies, Medicare and Medicaid as well as third party payors. The Administration has requested HHS and CMS issue proposed rules that may increase the scrutiny placed on companies that operate, directly or indirectly, multiple SNF and LTC facilities, and may subject our licensing and approval process to additional scrutiny or delays if such proposals are codified into regulations. If there are any delays in receiving regulatory approvals from the applicable federal, state or local government agencies, or the inability to receive such approvals, such delays could result in delayed or lost reimbursement related to periods of service prior to the receipt of such approvals, which could negatively impact our cash position.
48
Compliance with federal and state fair housing, fire, safety and other regulations may require us to make unanticipated expenditures, which could be costly to us.
We must comply with the federal Fair Housing Act and similar state laws, which prohibit us from discriminating against individuals if it would cause such individuals to face barriers in gaining residency in any of our affiliated facilities. Additionally, the Fair Housing Act and other similar state laws require that we advertise our services in such a way that we promote diversity and not limit it. We may be required, among other things, to change our marketing techniques to comply with these requirements.
In addition, we are required to operate our affiliated facilities in compliance with applicable fire and safety regulations, building codes and other land use regulations and food licensing or certification requirements as they may be adopted by governmental agencies and bodies from time to time. Like other healthcare facilities, our affiliated SNFs are subject to periodic surveys or inspections by governmental authorities to assess and assure compliance with regulatory requirements. Surveys occur on a regular (often annual or biannual) schedule, and special surveys may result from a specific complaint filed by a patient, a family member or one of our competitors. We may be required to make substantial capital expenditures to comply with these requirements.
We depend largely upon reimbursement from third-party payors, and our revenue, financial condition and results of operations could be negatively impacted by any changes in the acuity mix of patients in our affiliated facilities as well as payor mix and payment methodologies.
Our revenue is affected by the percentage of the patients of our operating subsidiaries who require a high level of skilled nursing and rehabilitative care, whom we refer to as high acuity patients, and by our mix of payment sources. Changes in the acuity level of patients we attract, as well as our payor mix among Medicaid, Medicare, private payors and managed care companies, significantly affect our profitability because we generally receive higher reimbursement rates for high acuity patients and because the payors reimburse us at different rates. For the years ended December 31, 2022 and 2021, 73.7% and 73.6%, of our revenue was provided by government payors that reimburse us at predetermined rates, respectively. If our labor or other operating costs increase, we will be unable to recover such increased costs from government payors. Accordingly, if we fail to maintain our proportion of high acuity patients or if there is any significant increase in the percentage of the patients of our operating subsidiaries for whom we receive Medicaid reimbursement, our results of operations may be adversely affected.
Initiatives undertaken by major insurers and managed care companies to contain healthcare costs may adversely affect our business. Among other initiatives, these payors attempt to control healthcare costs by contracting with healthcare providers to obtain services on a discounted basis. We believe that this trend will continue and may limit reimbursements for healthcare services. If insurers or managed care companies from whom we receive substantial payments were to reduce the amounts they pay for services, we may lose patients if we choose not to renew our contracts with these insurers at lower rates. Additionally, trade publications within the healthcare industry have reported on the recent trend of payors using the No Surprises Act as a means to force re-negotiation of reimbursement rates for providers and facilities. This trend has led to ongoing litigation between these providers and/or facilities against payors and it may adversely affect us as well.
On November 5, 2021, CMS issued the IFR discussed under Item 1., Government Regulation, subheading Coronavirus requiring all eligible staff to be fully vaccinated against COVID-19. CMS has been empowered to enforce the IFR nationwide and require compliance with its vaccination requirements since March 21, 2022.
In the event we or our affiliated facilities do not comply with the IFR, our Medicare and Medicaid agreements could be terminated and the termination of those agreements may lead to other payors terminating their agreements with us or our affiliated facilities and operating subsidiaries, which would materially and adversely affect our business, financial condition and results of operations.
In addition to the IFR, the Administration has requested HHS and CMS conduct studies about additional requirements pertaining to staffing, data reporting, employee compensation and retention, and resident experience that may result in a reduction of our revenue from Medicare and Medicaid. CMS issued its first proposed rule seeking information regarding these priorities in 2022 and subsequently published requests for information from the public in the Federal Register to aid in ongoing or future studies and anticipated rulemaking. These study results may result in additional conditions of participation within those programs.
49
We are subject to litigation that could result in significant legal costs and large settlement amounts or damage awards.
The skilled nursing business involves a significant risk of liability given the age and health of the patients and residents of our operating subsidiaries and the services we provide. The industry has experienced an increased trend in the number and severity of litigation claims, due in part to the number of large verdicts, including large punitive damage awards. These claims are filed based upon a wide variety of claims and theories, including deficiencies under conditions of participation under certain state and federal healthcare programs. Plaintiffs' attorneys have become increasingly more aggressive in their pursuit of claims against healthcare providers, including skilled nursing providers, employing a wide variety of advertising and solicitation activities to generate more claims. The increased caps on damages awarded in such actions, as discussed above, may trigger a larger number of these lawsuits against our independent operating subsidiaries in California and other states where we operate if they adopt similar legislation. The defense of lawsuits has in the past, and may in the future, result in significant legal costs, regardless of the outcome. Additionally, increases to the frequency and/or severity of losses from such claims and suits may result in increased liability insurance premiums or a decline in available insurance coverage levels, which could materially and adversely affect our business, financial condition and results of operations.
We have in the past been subject to class action litigation involving claims of violations of various regulatory requirements. While we have been able to settle these claims without an ongoing material adverse effect on our business, future claims could be brought that may materially affect our business, financial condition and results of operations. Other claims and suits, including class actions, continue to be filed against us and other companies in our industry. For example, there has been a general increase in the number of wage and hour class action claims filed in several of the jurisdictions where we are present. Allegations typically include claimed failures to permit or properly compensate for meal and rest periods, or failure to pay for time worked. If there were a significant increase in the number of these claims against us or an increase in amounts owing should plaintiffs be successful in their prosecution of these claims, this could have a material adverse effect to our business, financial condition, results of operations and cash flows.
Beyond our skilled nursing business, we engage in numerous ancillary businesses through one or more of our subsidiaries. These ancillary businesses generally support and provide services complementary to our operations, including but not limited to non-emergent ground transportation for patients and residents of our facilities. Our ancillary businesses may also be the subject of claims, lawsuits, and regulatory oversight that are specific to the particular services they offer. Noncompliance with the laws and regulations that may apply to our ancillary businesses may result in fines, penalties, and civil claims paid by our affected independent subsidiaries. Specific to our non-emergent ground transportation business, the drivers employed by this business may be subject to additional state-specific regulations regarding working time allowed to be spent driving, waiting time, and break or rest periods, and violations of these rules may lead to regulatory fines, penalties, or claims to be paid to individual drivers, in addition to the general employment risks described above.
Our ancillary businesses also are susceptible to general liability claims based on facts and circumstances that are specific to their activities and operations. In the case of our non-emergent ground transportation business, this liability likely exists in the form of automobile-involved accidents, which may involve property, individuals, or other automobiles. The defense of automobile accident and general liability lawsuits relating to our ancillary businesses in the past, and may in the future, result in significant legal costs, regardless of the outcome. As our ancillary businesses grow, the independent subsidiaries may be subject to increased frequency and/or severity of losses from such claims and suits which may result in increased liability insurance premiums for those businesses or a decline in available insurance coverage levels, which could materially and adversely affect our business, financial condition and results of operations.
In addition, we contract with a variety of landlords, lenders, vendors, suppliers, consultants and other individuals and businesses. These contracts typically contain covenants and default provisions. If the other party to one or more of our contracts were to allege that we have violated the contract terms, we could be subject to civil liabilities which could have a material adverse effect on our financial condition and results of operations.
If litigation is instituted against one or more of our subsidiaries, a successful plaintiff might attempt to hold us or another subsidiary liable for the alleged wrongdoing of the subsidiary principally targeted by the litigation. If a court in such litigation decided to disregard the corporate form, the resulting judgment could increase our liability and adversely affect our financial condition and results of operations.
50
Congress has repeatedly considered, without passage, a bill that would require, among other things, that agreements to arbitrate nursing home disputes be made after the dispute has arisen rather than before prospective patients move in, to prevent nursing home operators and prospective patients from mutually entering into a pre-admission pre-dispute arbitration agreement. This bill, known as the Fairness in Nursing Home Arbitration Act, was introduced in the House of Representatives in 2021; as of December 31, 2022, neither bill made it out of the committees to which it was referred for discussion to be voted on by the entire House of Representatives. Our independently operating subsidiaries use arbitration agreements, which have generally been favored by the courts, to streamline the dispute resolution process and reduce our exposure to legal fees and excessive jury awards. CMS has identified these arbitration agreements as an area for further review and issued guidance to state surveyors regarding arbitration agreements and their requirements under federal regulations, with non-compliance potentially resulting in fines and other sanctions. If we are not able to secure pre-admission arbitration agreements, our litigation exposure and costs of defense in patient liability actions could increase, our liability insurance premiums could increase, and our business may be adversely affected.
We conduct regular internal investigations into the care delivery, recordkeeping and billing processes of our operating subsidiaries. These reviews sometimes detect instances of noncompliance which we attempt to correct, which can decrease our revenue.
As an operator of healthcare facilities, we have a program to help us comply with various requirements of federal and private healthcare programs. Our compliance program includes, among other things, (i) policies and procedures modeled after applicable laws, regulations, government manuals and industry practices and customs that govern the clinical, reimbursement and operational aspects of our subsidiaries; (ii) training about our compliance process for all of the employees of our operating subsidiaries, our directors and officers, and training about Medicare and Medicaid laws, fraud and abuse prevention, clinical standards and practices, and claim submission and reimbursement policies and procedures for appropriate employees; and (iii) internal controls that monitor, for example, the accuracy of claims, reimbursement submissions, cost reports and source documents, provision of patient care, services, and supplies as required by applicable standards and laws, accuracy of clinical assessment and treatment documentation, and implementation of judicial and regulatory requirements (i.e., background checks, licensing and training).
From time to time our systems and controls highlight potential compliance issues, which we investigate as they arise. Historically, we have, and would continue to do so in the future, initiated internal inquiries into possible recordkeeping and related irregularities at our affiliated SNFs, which were detected by our internal compliance team in the course of its ongoing reviews.
Through these internal inquiries, we have identified potential deficiencies in the assessment of and recordkeeping for small subsets of patients. We have also identified and, at the conclusion of such investigations, assisted in implementing, targeted improvements in the assessment and recordkeeping practices to make them consistent with the existing standards and policies applicable to our affiliated SNFs in these areas. We continue to monitor the measures implemented for effectiveness and perform follow-up reviews to ensure compliance. Consistent with healthcare industry accounting practices, we record any charge for refunded payments against revenue in the period in which the claim adjustment becomes known.
If additional reviews result in identification and quantification of additional amounts to be refunded, we will accrue additional liabilities for claim costs and interest, and repay any amounts due in normal course. Furthermore, failure to refund overpayments within required time frames (as described in greater detail above) could result in FCA liability. If future investigations ultimately result in findings of significant billing and reimbursement noncompliance which could require us to record significant additional provisions or remit payments, our business, financial condition and results of operations could be materially and adversely affected and our stock price could decline.
We may be unable to complete future facility or business acquisitions at attractive prices or at all, which may adversely affect our revenue; we may also elect to dispose of underperforming or non-strategic operating subsidiaries, which would also decrease our revenue.
To date, our revenue growth has been significantly impacted by our acquisition of new facilities and businesses. Subject to general market conditions and the availability of essential resources and leadership within our company, we continue to seek both single-and multi-facility acquisition and business acquisition opportunities that are consistent with our geographic, financial and operating objectives.
51
We face competition for the acquisition of facilities and businesses and expect this competition to increase. Based upon factors such as our ability to identify suitable acquisition candidates, future regulations affecting the ability to purchase facilities, the purchase price of the facilities, increasing interest rates for debt-financed purchases, prevailing market conditions, the availability of leadership to manage new facilities and our own willingness to take on new operations, the rate at which we have historically acquired facilities has fluctuated significantly. In the future, we anticipate the rate at which we may acquire facilities will continue to fluctuate, which may affect our revenue.
We have also historically acquired a few facilities, which were or have proven to be non-strategic or less desirable, and we may consider disposing of such facilities or exchanging them for facilities which are more desirable, either because they were included in larger, indivisible groups of facilities or under other circumstances. To the extent we dispose of such a facility without simultaneously acquiring a facility in exchange, our revenue may decrease.
We may not be able to successfully integrate acquired facilities and businesses into our operations, and we may not achieve the benefits we expect from any of our facility acquisitions.
We may not be able to successfully or efficiently integrate new acquisitions of facilities and businesses with our existing operating subsidiaries, culture and systems. The process of integrating acquisitions into our existing operations may result in unforeseen operating difficulties, divert management's attention from existing operations, or require an unexpected commitment of staff and financial resources, and may ultimately be unsuccessful. Existing operations available for acquisition frequently serve or target different markets than those that we currently serve. We also may determine that renovations of acquired facilities and changes in staff and operating management personnel are necessary to successfully integrate those acquisitions into our existing operations. We may not be able to recover the costs incurred to reposition or renovate newly operating subsidiaries. The financial benefits we expect to realize from many of our acquisitions are largely dependent upon our ability to improve clinical performance, overcome regulatory deficiencies, rehabilitate or improve the reputation of the operations in the community, increase and maintain occupancy, control costs, and in some cases change the patient acuity mix. If we are unable to accomplish any of these objectives at the operating subsidiaries we acquire, we will not realize the anticipated benefits and we may experience lower than anticipated profits, or even losses.
During the year ended December 31, 2022, we expanded our operations through a combination of long-term leases and real estate purchases, with the addition of twenty-three stand-alone skilled nursing operations and one campus operation. In addition, we added five senior living operations that were transferred from Pennant, three of which are part of campuses operated by our affiliated operating subsidiaries. This growth has placed and will continue to place significant demands on our current management resources. Our ability to manage our growth effectively and to successfully integrate new acquisitions into our existing business will require us to continue to expand our operational, financial and management information systems and to continue to retain, attract, train, motivate and manage key employees, including facility-level leaders and our local directors of nursing. We may not be successful in attracting qualified individuals necessary for future acquisitions to be successful, and our management team may expend significant time and energy working to attract qualified personnel to manage facilities we may acquire in the future. Also, the newly acquired facilities may require us to spend significant time improving services that have historically been substandard, and if we are unable to improve such facilities quickly enough, we may be subject to litigation and/or loss of licensure or certification. If we are not able to successfully overcome these and other integration challenges, we may not achieve the benefits we expect from any of our acquisitions, and our business may suffer.
In undertaking acquisitions, we may be adversely impacted by costs, liabilities and regulatory issues that may adversely affect our operations.
In undertaking acquisitions, we also may be adversely impacted by unforeseen liabilities attributable to the prior providers who operated those facilities, against whom we may have little or no recourse. Many facilities we have historically acquired were underperforming financially and had clinical and regulatory issues prior to and at the time of acquisition. Even where we have improved operating subsidiaries and patient care at affiliated facilities that we have acquired, we still may face post-acquisition regulatory issues related to pre-acquisition events. These may include, without limitation, payment recoupment related to our predecessors' prior noncompliance, the imposition of fines, penalties, operational restrictions or special regulatory status. Further, we may incur post-acquisition compliance risk due to the difficulty or impossibility of immediately or quickly bringing non-compliant facilities into full compliance. Diligence materials pertaining to acquisition targets, especially the underperforming facilities that often represent the greatest opportunity for return, are often inadequate, inaccurate or impossible to obtain, sometimes requiring us to make acquisition decisions with incomplete information. Despite our due diligence procedures, facilities that we have acquired or may acquire in the future may generate unexpectedly low returns, may cause us to incur substantial losses, may require unexpected levels of management time, expenditures or other resources, or may otherwise not meet a risk profile that our investors find acceptable.
52
In addition, we might encounter unanticipated difficulties and expenditures relating to any of the acquired facilities, including contingent liabilities. For example, when we acquire a facility, we generally assume the facility's existing Medicare provider number for purposes of billing Medicare for services. If CMS later determines that the prior owner of the facility had received overpayments from Medicare for the period of time during which it operated the facility, or had incurred fines in connection with the operation of the facility, CMS could hold us liable for repayment of the overpayments or fines. We may be unable to improve every facility that we acquire. In addition, operation of these facilities may divert management time and attention from other operations and priorities, negatively impact cash flows, result in adverse or unanticipated accounting charges, or otherwise damage other areas of our company if they are not timely and adequately improved.
We also incur regulatory risk in acquiring certain facilities due to the licensing, certification and other regulatory requirements affecting our right to operate the acquired facilities. For example, in order to acquire facilities on a predictable schedule, or to acquire declining operations quickly to prevent further pre-acquisition declines, we frequently acquire such facilities prior to receiving license approval or provider certification. Anticipated future regulations may cause delays in acquiring the required licenses and certifications, if it is possible to do so at all. We operate such facilities as the interim manager for the outgoing licensee, assuming financial responsibility, among other obligations for the facility. To the extent that we may be unable or delayed in obtaining a license, we may need to operate the facility under a management agreement from the prior operator. Any inability in obtaining consent from the prior operator of a target acquisition to utilizing its license in this manner could impact our ability to acquire additional facilities. If we were subsequently denied licensure or certification for any reason, we might not realize the expected benefits of the acquisition and would likely incur unanticipated costs and other challenges which could cause our business to suffer.
If we do not achieve or maintain competitive quality of care ratings from CMS or private organizations engaged in similar monitoring activities, our business may be negatively affected.
As discussed in Item 1., under Government Regulation, CMS, as well as certain private organizations engaged in similar monitoring activities, provides comparative public data, rating every SNF operating in each state based upon quality-of-care indicators. CMS’s system is the Five-Star Quality Rating System, intended to compare nursing homes more easily. The Five-Star Quality Rating System gives each nursing home a rating of between one and five stars in various categories, with five-star ratings harder to obtain over time. The ratings are available on a consumer-facing website, Nursing Home Compare. In cases of acquisitions, the previous operator's clinical ratings are included in our overall Five-Star Quality Rating. Based on CMS guidance issued in June of 2022, it is expected that more data will be collected by CMS and ultimately reported on the Nursing Home Compare website. Similarly, due to CMS's June 2022 guidance, we expect CMS will seek to make the data reported on the Nursing Home Compare website more readily accessible and understandable for consumers.
CMS continues to increase quality measure thresholds, making it more difficult to achieve upward and five-star ratings. Most recently, CMS increased its quality measure thresholds in October of 2022, making it more difficult for facilities to obtain or maintain four- and five-star ratings. CMS has indicated that it will increase these quality measure thresholds every six months. CMS acknowledges that some facilities may see a decline in their overall five-star rating absent any new inspection information. This is relevant to our business because the five-star ratings of our affiliated facilities may decline even as their quality measures remain unchanged, or even if their quality measures improve. This change could further affect star ratings across the industry. Additionally, on the Nursing Home Compare website, CMS recently began displaying a consumer alert icon next to nursing homes that have been cited on inspection reports for incidents of abuse, neglect, or exploitation. In July of 2022, CMS updated the scoring measures used for SNFs to include six dimensions of staffing and turnover, which may affect the rating of our facilities on the Nursing Home Compare website. CMS’s expanded evaluation and measurement of staffing and turnover, including measures of all nurses, registered nurses, and administrators, may adversely affect the scoring and evaluation of our facilities under CMS’s Five-Star Quality Rating System. See Item 1., under Government Regulation.
Providing quality patient care is the cornerstone of our business. We believe that hospitals, physicians and other referral sources refer patients to us in large part because of our reputation for delivering quality care. If we should fail to achieve our internal rating goals or fail to exceed the national average rating on the Five-Star Quality Rating System, including due to nursing and administrative staffing and turnover, or have facilities displaying a consumer alert icon for incidents of abuse, neglect, or exploitation, it may affect our ability to generate referrals, which could have a material adverse effect upon our business and consolidated financial condition, results of operations and cash flows.
53
If we are unable to obtain insurance, or if insurance becomes more costly for us to obtain, our business may be adversely affected.
It may become more difficult and costly for us to obtain coverage for resident care liabilities and other risks, including property, automobile and casualty insurance. For example, the following circumstances may adversely affect our ability to obtain insurance at favorable rates:
•we experience higher-than-expected professional liability, property and casualty, or other types of claims or losses;
•we receive survey deficiencies or citations of higher-than-normal scope or severity;
•we acquire especially troubled operations or facilities that present unattractive risks to current or prospective insurers;
•insurers tighten underwriting standards applicable to us or our industry; or
•insurers or reinsurers are unable or unwilling to insure us or the industry at historical premiums and coverage levels.
If any of these potential circumstances were to occur, our insurance carriers may require us to significantly increase our self-insured retention levels or pay substantially higher premiums for the same or reduced coverage for insurance, including workers compensation, property and casualty, automobile, employment practices liability, directors and officers liability, employee healthcare and general and professional liability coverages.
In some states, the law prohibits or limits insurance coverage for the risk of punitive damages arising from professional liability and general liability claims or litigation. Coverage for punitive damages is also excluded under some insurance policies. As a result, we may be liable for punitive damage awards in these states that either are not covered or are in excess of our insurance policy limits. Claims against us, regardless of their merit or eventual outcome, also could inhibit our ability to attract patients or expand our business and could require our management to devote time to matters unrelated to the day-to-day operation of our business.
With few exceptions, workers compensation and employee health insurance costs have also increased markedly in recent years. To partially offset these increases, we have increased the amounts of our self-insured retention and deductibles in connection with general and professional liability claims. We also have implemented a self-insurance program for workers compensation in all states, except Washington, and elected non-subscriber status for workers compensation in Texas. In Washington, the insurance coverage is financed through premiums paid by the employers and employees. Due to the nature of our business and the residents we serve, including the risk of claims from residents as well as potential governmental action, it may be difficult to complete the underwriting process and obtain insurance at commercially reasonable rates. If we are unable to obtain insurance, or if insurance becomes more costly for us to obtain, or if the coverage levels we can economically obtain decline, our business may be adversely affected.
Our self-insurance programs may expose us to significant and unexpected costs and losses.
We have maintained general and professional liability insurance since 2002 and workers compensation insurance since 2005 through a wholly-owned captive insurance subsidiary to insure our self-insurance reimbursements and deductibles as part of a continually evolving overall risk management strategy. We establish the insurance loss reserves based on an estimation process that uses information obtained from both company-specific and industry data. The estimation process requires us to continuously monitor and evaluate the life cycle of the claims. Using data obtained from this monitoring and our assumptions about emerging trends, we, along with an independent actuary, develop information about the size of ultimate claims based on our historical experience and other available industry information. The most significant assumptions used in the estimation process include determining the trend in costs, the expected cost of claims incurred but not reported and the expected costs to settle or pay damages with respect to unpaid claims. It is possible, however, that the actual liabilities may exceed our estimates of loss. We may also experience an unexpectedly large number of successful claims or claims that result in costs or liability significantly in excess of our projections. For these and other reasons, our self-insurance reserves could prove to be inadequate, resulting in liabilities in excess of our available insurance and self-insurance. If a successful claim is made against us and it is not covered by our insurance or exceeds the insurance policy limits, our business may be negatively and materially impacted.
Further, because our self-insurance reimbursements under our general and professional liability and workers compensation programs applies on a per claim basis, there is no limit to the maximum number of claims or the total amount for which we could incur liability in any policy period.
54
We also self-insure our employee health benefits. With respect to our health benefits self-insurance, our reserves and premiums are computed based on a mix of company specific and general industry data that is not specific to our own company. Even with a combination of limited company-specific loss data and general industry data, our loss reserves are based on actuarial estimates that may not correlate to actual loss experience in the future. Therefore, our reserves may prove to be insufficient and we may be exposed to significant and unexpected losses.
The frequency and magnitude of claims and legal costs may increase due to the COVID-19 pandemic or our related response efforts.
The geographic concentration of our affiliated facilities could leave us vulnerable to an economic downturn, regulatory changes or acts of nature in those areas.
Our affiliated facilities located in Arizona, California, and Texas account for the majority of our total revenue. As a result of this concentration, the conditions of local economies, changes in governmental rules, regulations and reimbursement rates or criteria, changes in demographics, state funding, acts of nature and other factors that may result in a decrease in demand and/or reimbursement for skilled nursing services in these states could have a disproportionately adverse effect on our revenue, costs and results of operations. Moreover, since over 20% of our affiliated facilities are located in California, we are particularly susceptible to revenue loss, cost increase or damage caused by natural disasters such as electrical power shortages, fires, earthquakes or mudslides, or increased liabilities that may arise from regulations as discussed within Item 1., under Government Regulation.
In addition, our affiliated facilities in Iowa, Nebraska, Kansas, South Carolina, Washington and Texas are more susceptible to revenue loss, cost increases or damage caused by natural disasters including hurricanes, tornadoes and flooding. These acts of nature may cause disruption to us, the employees of our operating subsidiaries and our affiliated facilities, which could have an adverse impact on the patients of our operating subsidiaries and our business. In order to provide care for the patients of our operating subsidiaries, we are dependent on consistent and reliable delivery of food, pharmaceuticals, utilities and other goods to our affiliated facilities, and the availability of employees to provide services at our affiliated facilities. If the delivery of goods or the ability of employees to reach our affiliated facilities were interrupted in any material respect due to a natural disaster or other reasons, it would have a significant impact on our affiliated facilities and our business. Furthermore, the impact, or impending threat, of a natural disaster may require that we evacuate one or more facilities, which would be costly and would involve risks, including potentially fatal risks, for the patients. The impact of disasters and similar events is inherently uncertain. Such events could harm the patients and employees of our operating subsidiaries, severely damage or destroy one or more of our affiliated facilities, harm our business, reputation and financial performance, or otherwise cause our business to suffer in ways that we currently cannot predict.
The actions of a national labor union that has pursued a negative publicity campaign criticizing our business in the past may adversely affect our revenue and our profitability.
We continue to maintain our right to inform the employees of our operating subsidiaries about our views of the potential impact of unionization upon the workplace generally and upon individual employees. With one exception, to our knowledge the staff at our affiliated facilities that have been approached to unionize have uniformly rejected union organizing efforts. Forthcoming proposed rules from HHS and CMS, which, based on the Administration's statements and guidance since February of 2022, are anticipated within the next year, may increase the likelihood of employee unionization due to increased emphasis on care-based careers in SNFs and LTC facilities. If employees decide to unionize, our cost of doing business could increase, and we could experience contract delays, difficulty in adapting to a changing regulatory and economic environment, cultural conflicts between unionized and non-unionized employees, strikes and work stoppages, and we may conclude that affected facilities or operations would be uneconomical to continue operating.
Because we lease the majority of our affiliated facilities, we are subject to risks associated with leased real property, including risks relating to lease termination, lease extensions and special charges, any of which could adversely affect our business, financial position or results of operations.
As of December 31, 2022, we leased 192 of our 271 affiliated facilities. Most of our leases are triple-net leases, which means that, in addition to rent, we are required to pay for the costs related to the property (including property taxes, insurance, and maintenance and repair costs). We are responsible for paying these costs notwithstanding the fact that some of the benefits associated with paying these costs accrue to the landlords as owners of the associated facilities.
55
Each lease provides that the landlord may terminate the lease for a variety of reasons, including the default in any payment of rent, taxes or other payment obligations or the breach of any other covenant or agreement in the lease. Termination of a lease could result in a default under our debt agreements and could adversely affect our business, financial position or results of operations. There can be no assurance that we will be able to comply with all of our obligations under the leases in the future.
Failure to generate sufficient cash flow to cover required payments or meet operating covenants under our long-term debt, mortgages and long-term operating leases could result in defaults under such agreements and cross-defaults under other debt, mortgage or operating lease arrangements, which could harm our operating subsidiaries and cause us to lose facilities or experience foreclosures.
Our Amended Credit Agreement provides for a Revolving Credit Facility with borrowing capacity of up to $600.0 million in aggregate principal amount. As of December 31, 2022 and through the filing of this report, we had no outstanding borrowings under our Revolving Credit Facility. Twenty-three of our subsidiaries have mortgage loans insured with Department of Housing and Urban Development (HUD) for an aggregate amount of $153.5 million, which subjects these subsidiaries to HUD oversight and periodic inspections. The terms of the mortgage loans range from 25- to 35-years.
We also have two outstanding promissory notes with an aggregate principal amount of approximately $2.8 million as of December 31, 2022. The term of the notes are 10 months and 12 years. Because this mortgage loan is insured with HUD, our borrower subsidiary under the loan is subject to HUD oversight and periodic inspections.
In addition, we had $2.2 billion of future operating lease obligations as of December 31, 2022. We intend to continue financing our operating subsidiaries through mortgage financing, long-term operating leases and other types of financing, including borrowings under our lines of credit and future credit facilities we may obtain.
We may not generate sufficient cash flow from operations to cover required interest, principal and lease payments. In addition, our outstanding Amended Credit Agreement and mortgage loans contain restrictive covenants and require us to maintain or satisfy specified coverage tests on a consolidated basis and on a facility or facilities basis. These restrictions and operating covenants include, among other things, requirements with respect to occupancy, debt service coverage, project yield, net leverage ratios, minimum interest coverage ratios and minimum asset coverage ratios. These restrictions may interfere with our ability to obtain additional advances under our Revolving Credit Facility or to obtain new financing or to engage in other business activities, which may inhibit our ability to grow our business and increase revenue.
From time to time, the financial performance of one or more of our mortgaged facilities may not comply with the required operating covenants under the terms of the mortgage. Any non-payment, noncompliance or other default under our financing arrangements could, subject to cure provisions, cause the lender to foreclose upon the facility or facilities securing such indebtedness or, in the case of a lease, cause the lessor to terminate the lease, each with a consequent loss of revenue and asset value to us or a loss of property. Furthermore, in many cases, indebtedness is secured by both a mortgage on one or more facilities, and a guaranty by us. In the event of a default under one of these scenarios, the lender could avoid judicial procedures required to foreclose on real property by declaring all amounts outstanding under the guaranty immediately due and payable, and requiring us to fulfill our obligations to make such payments. If any of these scenarios were to occur, our financial condition would be adversely affected. For tax purposes, a foreclosure on any of our properties would be treated as a sale of the property for a price equal to the outstanding balance of the debt secured by the mortgage. If the outstanding balance of the debt secured by the mortgage exceeds our tax basis in the property, we would recognize taxable income on foreclosure, but would not receive any cash proceeds, which would negatively impact our earnings and cash position. Further, because our mortgages and operating leases generally contain cross-default and cross-collateralization provisions, a default by us related to one facility could affect a significant number of other facilities and their corresponding financing arrangements and operating leases.
56
Because our term loans, promissory notes, bonds, mortgages and lease obligations are fixed expenses and secured by specific assets, and because our revolving loan obligations are secured by virtually all of our assets, if reimbursement rates, patient acuity mix or occupancy levels decline, or if for any reason we are unable to meet our loan or lease obligations, we may not be able to cover our costs and some or all of our assets may become at risk. Our ability to make payments of principal and interest on our indebtedness and to make lease payments on our operating leases depends upon our future performance, which will be subject to general economic conditions, industry cycles and financial, business and other factors affecting our operating subsidiaries, many of which are beyond our control. If we are unable to generate sufficient cash flow from operations in the future to service our debt or to make lease payments on our operating leases, we may be required, among other things, to seek additional financing in the debt or equity markets, refinance or restructure all or a portion of our indebtedness, sell selected assets, reduce or delay planned capital expenditures or delay or abandon desirable acquisitions. Such measures might not be sufficient to enable us to service our debt or to make lease payments on our operating leases. The failure to make required payments on our debt or operating leases or the delay or abandonment of our planned growth strategy could result in an adverse effect on our future ability to generate revenue and sustain profitability. In addition, any such financing, refinancing or sale of assets might not be available on terms that are economically favorable to us, or at all.
Move-in and occupancy rates may remain unpredictable even after the COVID-19 pandemic is over.
Occupancy levels at SNFs are likely to remain vulnerable to the effects of COVID-19 even after the pandemic is over. Facilities experiencing decreases in move-in rates in 2021 cite resident or family member concerns as the basis for such decreases. These and other similar concerns may continue to impact our ability to attract new residents and our ability to retain existing residents.
A housing downturn could decrease demand for senior living services.
Seniors often use the proceeds of home sales to fund their admission to senior living facilities. A downturn in the housing markets, including reductions in sales prices caused by increasing mortgage interest rates, could adversely affect seniors’ ability to afford our resident fees and entrance fees. If national or local housing markets enter a persistent decline, our occupancy rates, revenues, results of operations and cash flow could be negatively impacted.
As we continue to acquire and lease real estate assets, we may not be successful in identifying and consummating these transactions.
As part of, and subsequent to the spin-off transaction in 2019, we lease 29 of our properties to Pennant’s senior living operations. In the future, we might expand our leasing property portfolio to additional Pennant operations or other unaffiliated tenants. We have very limited control over the success or failure of our tenants’ and operators’ businesses and, at any time, a tenant or operator may experience a downturn in its business that weakens its financial condition. If that happens, the tenant or operator may fail to make its payments to us when due. Although our lease agreements give us the right to exercise certain remedies in the event of default on the obligations owing to us, we may determine not to do so if we believe that enforcement of our rights would be more detrimental to our business than seeking alternative approaches.
An important part of our business strategy is to continue to expand and diversify our real estate portfolio through accretive acquisition and investment opportunities in healthcare properties. Our execution of this strategy by successfully identifying, securing and consummating beneficial transactions is made more challenging by increased competition and can be affected by many factors, including our relationships with current and prospective tenants, our ability to obtain debt and equity capital at costs comparable to or better than our competitors and our ability to negotiate favorable terms with property owners seeking to sell and other contractual counterparties. Our competitors for these opportunities include healthcare REITs, real estate partnerships, healthcare providers, healthcare lenders and other investors, including developers, banks, insurance companies, pension funds, government-sponsored entities and private equity firms, some of whom may have greater financial resources and lower costs of capital than we do. Potential regulations may affect the ability of these entities, as well as ourselves, to compete for these opportunities or enter into transactions for real estate related to our business. If we are unsuccessful at identifying and capitalizing on investment or acquisition opportunities, our growth and profitability in our real estate investment portfolio may be adversely affected.
57
Investments in and acquisitions of healthcare properties entail risks associated with real estate investments generally, including risks that the investment will not achieve expected returns, that the cost estimates for necessary property improvements will prove inaccurate or that the tenant or operator will fail to meet performance expectations. Income from properties and yields from investments in our properties may be affected by many factors, including changes in governmental regulation (such as licensing and government payment), general or local economic conditions (such as fluctuations in interest rates, senior savings, and employment conditions), the available local supply of and demand for improved real estate, a reduction in rental income as the result of an inability to maintain occupancy levels, natural disasters (such as hurricanes, earthquakes and floods) or similar factors. Furthermore, healthcare properties are often highly customized, and the development or redevelopment of such properties may require costly tenant-specific improvements. As a result, we cannot assure you that we will achieve the economic benefit we expect from acquisition or investment opportunities.
As we expand our presence in other relevant healthcare industries, we would become subject to risks in a market in which we have limited experience.
The majority of our affiliated facilities have historically been SNFs. As we expand our presence in other relevant healthcare industries, our existing overall business model will continue to change and expose our company to risks in markets in which we have limited experience. We expect that we will have to adjust certain elements of our existing business model, which could have an adverse effect on our business.
If our referral sources fail to view us as an attractive skilled nursing provider, or if our referral sources otherwise refer fewer patients, our patient base may decrease.
We rely significantly on appropriate referrals from physicians, hospitals and other healthcare providers in the communities in which we deliver our services to attract appropriate residents and patients to our affiliated facilities. Our referral sources are not obligated to refer business to us and may refer business to other healthcare providers. We believe many of our referral sources refer business to us as a result of the quality of our patient care and our efforts to establish and build a relationship with our referral sources. If we lose, or fail to maintain, existing relationships with our referral resources, fail to develop new relationships, or if we are perceived by our referral sources as not providing high quality patient care, our occupancy rate and the quality of our patient mix could suffer. In addition, if any of our referral sources have a reduction in patients whom they can refer due to a decrease in their business, our occupancy rate and the quality of our patient mix could suffer.
We may need additional capital to fund our operating subsidiaries and finance our growth, and we may not be able to obtain it on terms acceptable to us, or at all, which may limit our ability to grow.
Our ability to maintain and enhance our operating subsidiaries and equipment in a suitable condition to meet regulatory standards, operate efficiently and remain competitive in our markets requires us to commit substantial resources to continued investment in our affiliated facilities and equipment. We are sometimes more aggressive than our competitors in capital spending to address issues that arise in connection with aging and obsolete facilities and equipment. In addition, continued expansion of our business through the acquisition of existing facilities, expansion of our existing facilities and construction of new facilities may require additional capital, particularly if we were to accelerate our acquisition and expansion plans. Financing may not be available to us or may be available to us only on terms that are not favorable, including being subject to interest rates that are higher than those incurred in the recent past. In addition, some of our outstanding indebtedness and long-term leases restrict, among other things, our ability to incur additional debt. If we are unable to raise additional funds or obtain additional funds on terms acceptable to us, we may have to delay or abandon some or all of our growth strategies. Further, if additional funds are raised through the issuance of additional equity securities, the percentage ownership of our stockholders would be diluted. Any newly issued equity securities may have rights, preferences or privileges senior to those of our common stock.
58
The condition of the financial markets, including volatility and deterioration in the capital and credit markets, could limit the availability of debt and equity financing sources to fund the capital and liquidity requirements of our business, as well as negatively impact or impair the value of our current portfolio of cash, cash equivalents and investments, including U.S. Treasury securities and U.S.-backed investments.
Our cash, cash equivalents and investments are held in a variety of interest-bearing instruments, including U.S. treasury securities. As a result of the uncertain domestic and global political, economic, credit and financial market conditions, including the recent significant increase in the federal funds rate, an increase in the Consumer Price Index of seven percent in 2021, which has continued at a comparable rate for 2022, investments in these types of financial instruments pose risks arising from liquidity and credit concerns. Given that future deterioration in the U.S. and global credit and financial markets is a possibility, no assurance can be made that losses or significant deterioration in the fair value of our cash, cash equivalents, or investments will not occur. Uncertainty surrounding the trading market for U.S. government securities or impairment of the U.S. government's ability to satisfy its obligations under such treasury securities could impact the liquidity or valuation of our current portfolio of cash, cash equivalents, and investments, a substantial portion of which were invested in U.S. treasury securities. Further, continued domestic and international political uncertainty, along with credit, and financial market uncertainty, may make it difficult for us to liquidate our investments prior to their maturity without incurring a loss, which would have a material adverse effect on our consolidated financial position, results of operations or cash flows.
We may need additional capital if a substantial acquisition or other growth opportunity becomes available or if unexpected events occur or opportunities arise. U.S. capital markets can be volatile. We cannot assure you that additional capital will be available or available on terms acceptable to us. If capital is not available, we may not be able to fund internal or external business expansion or respond to competitive pressures or other market conditions.
Delays in reimbursement may cause liquidity problems.
If we experience problems with our billing information systems or if issues arise with Medicare, Medicaid or other payors, including attempts by commercial health insurance companies to renegotiate rates by reducing or withholding payment, we may encounter delays in our payment cycle. From time to time, we have experienced such delays as a result of government payors instituting planned reimbursement delays for budget balancing purposes or as a result of prepayment reviews.
Some states in which we operate are operating with budget deficits or could have budget deficit in the future, which may delay reimbursement in a manner that would adversely affect our liquidity. In addition, from time to time, procedural issues require us to resubmit or appeal claims before payment is remitted, which contributes to our aged receivables. Unanticipated delays in receiving reimbursement from state programs due to changes in their policies or billing or audit procedures may adversely impact our liquidity and working capital.
The continued use and growth of Medicaid managed care organizations (MCOs) may contribute to delays or reductions in our Medicaid reimbursement.
In forty-one states, including some of the largest where we operate, state Medicaid benefits are administered through MCOs. Typically, these MCOs are also commercial health insurers that administer state Medicaid benefits under a managed care contract. Nationally, MCOs cover approximately 57 million Medicaid beneficiaries. Due to these MCOs’ experience in healthcare reimbursement, they may be more aggressive than state Medicaid agencies in denying claims or seeking recoupment of payments so that their services under these managed contracts are profitable. Additionally, the transfer of funds from state Medicaid agencies to these MCOs for disbursement may cause further delays in payment. The additional steps created by the use of MCOs in disbursement of Medicaid funds creates more risk of delayed, reduced, or recouped payments for our independent operating subsidiaries, and additional avenues for risks that include fines and other sanctions, including suspension or exclusion from participation in state Medicaid programs.
59
Compliance with the regulations of the Department of Housing and Urban Development may require us to make unanticipated expenditures which could increase our costs.
Twenty-three of our affiliated facilities are currently subject to regulatory agreements with HUD that give the Commissioner of HUD broad authority to require us to be replaced as the operator of those facilities in the event that the Commissioner determines there are operational deficiencies at such facilities under HUD regulations. Compliance with HUD's requirements can often be difficult because these requirements are not always consistent with the requirements of other federal and state agencies. Appealing a failed inspection can be costly and time-consuming and, if we do not successfully remediate the failed inspection, we could be precluded from obtaining HUD financing in the future or we may encounter limitations or prohibitions on our operation of HUD-insured facilities.
If we fail to safeguard the monies held in our patient trust funds, we will be required to reimburse such monies, and we may be subject to citations, fines and penalties.
Each of our affiliated facilities is required by federal law to maintain a patient trust fund to safeguard certain assets of their residents and patients. If any money held in a patient trust fund is misappropriated, we are required to reimburse the patient trust fund for the amount of money that was misappropriated. If any monies held in our patient trust funds are misappropriated in the future and are unrecoverable, we will be required to reimburse such monies, and we may be subject to citations, fines and penalties pursuant to federal and state laws.
We are a holding company with no operations and rely upon our multiple independent operating subsidiaries to provide us with the funds necessary to meet our financial obligations. Liabilities of any one or more of our subsidiaries could be imposed upon us or our other subsidiaries.
We are a holding company with no direct operating assets, employees or revenue. Each of our affiliated facilities is operated through a separate, wholly-owned, independent subsidiary, which has its own management, employees and assets. Our principal assets are the equity interests we directly or indirectly hold in our multiple operating and real estate holding subsidiaries. As a result, we are dependent upon distributions from our subsidiaries to generate the funds necessary to meet our financial obligations and pay dividends. Our subsidiaries are legally distinct from us and have no obligation to make funds available to us. The ability of our subsidiaries to make distributions to us will depend substantially on their respective operating results and will be subject to restrictions under, among other things, the laws of their jurisdiction of organization, which may limit the amount of funds available for distribution to investors or stockholders, agreements of those subsidiaries, the terms of our financing arrangements and the terms of any future financing arrangements of our subsidiaries.
If the separation of Pennant fails to qualify as generally tax-free for U.S. federal income tax purposes, we and our stockholders could be subject to significant tax liabilities.
The spin-off in 2019 is intended to qualify for tax-free treatment to us and our stockholders for U.S. federal income tax purposes. Accordingly, completion of the transaction was conditioned upon, among other things, our receipt of opinions from outside tax advisors that the distributions would qualify as a transaction that is intended to be tax-free to both us and our stockholders for U.S. federal income tax purposes under Sections 355 and 368(a)(1)(D) of the Internal Revenue Code. The opinions were based on and relied on, among other things, certain facts and assumptions, as well as certain representations, statements and undertakings, including those relating to the past and future conduct. If any of these facts, assumptions, representations, statements or undertakings is, or becomes, inaccurate or incomplete, or if any of the parties breach any of their respective covenants relating to the transactions, the tax opinions may be invalid. Moreover, the opinions are not binding on the IRS or any courts. Accordingly, notwithstanding receipt of the opinion, the IRS could determine that the distribution and certain related transactions should be treated as taxable transactions for U.S. federal income tax purposes.
If the spin-off fails to qualify as a transaction that is generally tax-free under Sections 355 and 368(a)(1)(D) of the Internal Revenue Code, in general, for U.S. federal income tax purposes, we would recognize taxable gain with respect to the distributed securities and our stockholders who received securities in such distribution would be subject to tax as if they had received a taxable distribution equal to the fair market value of such shares.
We also have obligations to provide indemnification to a number of parties as a result of the transaction. Any indemnity obligations for tax issues or other liabilities related to the spin-off, could be significant and could adversely impact our business.
60
Certain directors who serve on our Board of Directors also serve as directors of Pennant, and ownership of shares of Pennant common stock by our directors and executive officers may create, or appear to create, conflicts of interest.
Certain of our directors who serve on our Board of Directors also serve on the board of directors of Pennant. This may create, or appear to create, conflicts of interest when our, or Pennant's management and directors face decisions that could have different implications for us and Pennant, including the resolution of any dispute regarding the terms of the agreements governing the spin-off and the relationship between us and Pennant after the spin-off or any other commercial agreements entered into in the future between us and the spun-off business and the allocation of such directors’ time between us and Pennant.
All of our executive officers and some of our non-employee directors own shares of the common stock of Pennant. The continued ownership of such common stock by our directors and executive officers following the spin-off creates, or may create, the appearance of a conflict of interest when these directors and executive officers are faced with decisions that could have different implications for us and Pennant.
If Standard Bearer fails to qualify or remain qualified as a REIT, it will be subject to U.S. federal income tax as a regular corporation and could face substantial tax liability.
Standard Bearer currently operates, and intends to continue to operate, in a manner that will allows it to qualify to be taxed as a REIT for U.S. federal income tax purposes. Standard Bearer intends to elect to be taxed as a REIT for U.S. federal income tax purposes beginning with its taxable year ended December 31, 2022.
If Standard Bearer fails to qualify to be taxed as a REIT in any year, it would be subject to U.S. federal income tax, including any applicable alternative minimum tax, on our taxable income at regular corporate rates, and dividends paid to its shareholders would not be deductible by it in computing its taxable income. Any resulting corporate liability could be substantial and would reduce the amount of cash available for distribution to its shareholders. Unless it was entitled to relief under certain Code provisions, it also would be disqualified from re-electing to be taxed as a REIT for the four taxable years following the year in which it failed to qualify to be taxed as a REIT.
Legislative or other actions affecting REITs could have a negative effect on Standard Bearer.
The rules dealing with U.S. federal income taxation are constantly under review by persons involved in the legislative process and by the IRS and the U.S. Department of the Treasury (the “Treasury”). Changes to the tax laws or interpretations thereof, with or without retroactive application, could materially and adversely affect Standard Bearer's investors or Standard Bearer. We cannot predict how changes in the tax laws, including any tax reform called for by the current presidential administration, might affect Standard Bearer or its investors. New legislation, Treasury regulations, administrative interpretations or court decisions could significantly and negatively affect its ability to qualify to be taxed as a REIT or the U.S. federal income tax consequences to Standard Bearer or its investors of such qualification. For instance, the “Tax Cuts and Jobs Act” (the “Act”) significantly changed the U.S. federal income tax laws applicable to businesses and their owners, including REITs and their shareholders. Technical corrections or other amendments to the Act or administrative guidance interpreting the Act may be forthcoming at any time. We cannot predict the long-term effect of the Act or any future law changes on REITs or their shareholders. Changes to the U.S. federal tax laws and interpretations thereof, whether under the Act or otherwise, could adversely affect an investment in our stock.
No prediction can be made regarding whether new legislation or regulation (including new tax measures) will be enacted by legislative bodies or governmental agencies, nor can we predict what consequences would result from this legislation or regulation. Accordingly, no assurance can be given that the currently anticipated tax treatment of an investment will not be modified by legislative, judicial or administrative changes, possibly with retroactive effect.
Standard Bearer could fail to qualify to be taxed as a REIT if income it receives from our tenants is not treated as qualifying income.
Under applicable provisions of the Code, Standard Bearer will not be treated as a REIT unless it satisfies various requirements, including requirements relating to the sources of its gross income. Rents received or accrued by it from its tenants will not be treated as qualifying rent for purposes of these requirements if the leases are not respected as true leases for U.S. federal income tax purposes and are instead treated as service contracts, joint ventures or other arrangements. If the leases are not respected as true leases for U.S. federal income tax purposes, Standard Bearer will likely fail to qualify to be taxed as a REIT.
61
Even if Standard Bearer remains qualified as a REIT, it may face other tax liabilities that reduce its cash flow.
Even if Standard Bearer remain qualified for taxation as a REIT, it may be subject to certain U.S. federal, state, and local taxes on its income and assets, including taxes on any undistributed income and state or local income, property and transfer taxes. For example, Standard Bearer may hold some of its assets or conduct certain of its activities through one or more taxable REIT subsidiaries (each, a “TRS”) or other subsidiary corporations that will be subject to U.S. federal, state, and local corporate-level income taxes as regular C corporations. In addition, it may incur a 100% excise tax on transactions with a TRS if they are not conducted on an arm’s-length basis. Any of these taxes would decrease cash available for distribution to its shareholders.
Risks Related to Ownership of our Common Stock
We may not be able to pay or maintain dividends and the failure to do so would adversely affect our stock price.
Our ability to pay and maintain cash dividends is based on many factors, including our ability to make and finance acquisitions, our ability to negotiate favorable lease and other contractual terms, anticipated operating cost levels, the level of demand for our beds, the rates we charge and actual results that may vary substantially from estimates. Some of the factors are beyond our control and a change in any such factor could affect our ability to pay or maintain dividends. The Amended Credit Agreement restricts our ability to pay dividends to stockholders if we receive notice that we are in default under this agreement. The failure to pay or maintain dividends could adversely affect our stock price.
Our amended and restated certificate of incorporation, amended and restated bylaws and Delaware law contain provisions that could discourage transactions resulting in a change in control, which may negatively affect the market price of our common stock.
Our amended and restated certificate of incorporation and our amended and restated bylaws contain provisions that may enable our Board of Directors to resist a change in control. These provisions may discourage, delay or prevent a change in the ownership of our company or a change in our management, even if doing so might be beneficial to our stockholders. In addition, these provisions could limit the price that investors would be willing to pay in the future for shares of our common stock. Such provisions set forth in our amended and restated certificate of incorporation or our amended and restated bylaws include:
•our Board of Directors is authorized, without prior stockholder approval, to create and issue preferred stock, commonly referred to as “blank check” preferred stock, with rights senior to those of common stock;
•advance notice requirements for stockholders to nominate individuals to serve on our Board of Directors or to submit proposals that can be acted upon at stockholder meetings;
•our Board of Directors is classified so not all members of our board are elected at one time, which may make it more difficult for a person who acquires control of a majority of our outstanding voting stock to replace our directors;
•stockholder action by written consent is limited;
•special meetings of the stockholders are permitted to be called only by the chairman of our Board of Directors, our chief executive officer or by a majority of our Board of Directors;
•stockholders are not permitted to cumulate their votes for the election of directors;
•newly created directorships resulting from an increase in the authorized number of directors or vacancies on our Board of Directors are filled only by majority vote of the remaining directors;
•our Board of Directors is expressly authorized to make, alter or repeal our bylaws; and
•stockholders are permitted to amend our bylaws only upon receiving the affirmative vote of at least a majority of our outstanding common stock.
We are also subject to the anti-takeover provisions of Section 203 of the General Corporation Law of the State of Delaware. Under these provisions, if anyone becomes an “interested stockholder,” we may not enter into a “business combination” with that person for three years without special approval, which could discourage a third party from making a takeover offer and could delay or prevent a change of control. For purposes of Section 203, “interested stockholder” means, generally, someone owning more than 15% or more of our outstanding voting stock or an affiliate of ours that owned 15% or more of our outstanding voting stock during the past three years, subject to certain exceptions as described in Section 203.
62
These and other provisions in our amended and restated certificate of incorporation, amended and restated bylaws and Delaware law could discourage acquisition proposals and make it more difficult or expensive for stockholders or potential acquirers to obtain control of our Board of Directors or initiate actions that are opposed by our then-current Board of Directors, including delaying or impeding a merger, tender offer or proxy contest involving us. Any delay or prevention of a change of control transaction or changes in our Board of Directors could cause the market price of our common stock to decline.
Item 1B. UNRESOLVED STAFF COMMENTS
None.
Item 2. PROPERTIES
Service Center — Our Service Center is located in San Juan Capistrano, California. In June 2018, we acquired an office space for a purchase price of $31.0 million to accommodate our growing Service Center team. The property consists of approximately 108,058 square feet of usable office space. In addition, we lease a substantial portion of the space within the campus to third-party tenants. Additionally, in 2022, we entered into lease agreements for office space in Texas and Utah as we expanded our Service Centers in those states.
Operating Facilities — We operate 271 affiliated facilities in Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin, with the operational capacity to serve approximately 31,000 patients as of December 31, 2022. Of the 271 facilities, we operate 192 facilities under long-term lease arrangements and have options to purchase 11 of those 192 facilities. The results of our operating facilities are reflected in our skilled services segment for our skilled nursing operations and in "All Other" category for our senior living operations.
The following table provides summary information regarding the location of our facilities, operational beds and units by property type as of December 31, 2022:
| Operated Facilities | |||||||||||||||||||||||||||||||||||
| Leased without a Purchase Option | Leased with a Purchase Option | Owned | Total | ||||||||||||||||||||||||||||||||
| Facilities | Beds/Units | Facilities | Beds/Units | Facilities | Beds/Units | Facilities | Beds/Units | ||||||||||||||||||||||||||||
| California | 42 | 4,269 | — | — | 11 | 1,224 | 53 | 5,493 | |||||||||||||||||||||||||||
| Texas | 56 | 6,932 | 5 | 714 | 21 | 2,711 | 82 | 10,357 | |||||||||||||||||||||||||||
| Arizona | 23 | 3,324 | — | — | 13 | 1,942 | 36 | 5,266 | |||||||||||||||||||||||||||
| Wisconsin | — | — | — | — | 2 | 100 | 2 | 100 | |||||||||||||||||||||||||||
| Utah | 12 | 1,311 | 2 | 159 | 7 | 684 | 21 | 2,154 | |||||||||||||||||||||||||||
| Colorado | 14 | 1,366 | 1 | 125 | 7 | 822 | 22 | 2,313 | |||||||||||||||||||||||||||
| Washington | 12 | 1,121 | — | — | 2 | 204 | 14 | 1,325 | |||||||||||||||||||||||||||
| Idaho | 7 | 551 | — | — | 5 | 468 | 12 | 1,019 | |||||||||||||||||||||||||||
| Nebraska | 5 | 364 | — | — | 2 | 354 | 7 | 718 | |||||||||||||||||||||||||||
| Kansas | — | — | 3 | 325 | 4 | 458 | 7 | 783 | |||||||||||||||||||||||||||
| Iowa | 6 | 399 | — | — | — | — | 6 | 399 | |||||||||||||||||||||||||||
| South Carolina | 2 | 322 | — | — | 5 | 544 | 7 | 866 | |||||||||||||||||||||||||||
| Nevada | 2 | 358 | — | — | — | — | 2 | 358 | |||||||||||||||||||||||||||
| 181 | 20,317 | 11 | 1,323 | 79 | 9,511 | 271 | 31,151 | ||||||||||||||||||||||||||||
63
The following table sets forth the location of our facilities and the number of operational beds and units located at our skilled nursing, senior living and campus facilities as of December 31, 2022:
| Facility Counts | Bed / Unit Counts | |||||||||||||||||||||||||
| Skilled Nursing Operations | Senior Living Communities | Campus Operations | Total | Skilled Nursing Beds | Senior Living Units | Total Beds / Units | ||||||||||||||||||||
| California | 50 | — | 3 | 53 | 5,296 | 197 | 5,493 | |||||||||||||||||||
| Texas | 77 | 1 | 4 | 82 | 9,848 | 509 | 10,357 | |||||||||||||||||||
| Arizona | 30 | 1 | 5 | 36 | 4,507 | 759 | 5,266 | |||||||||||||||||||
| Wisconsin | 2 | — | — | 2 | 100 | — | 100 | |||||||||||||||||||
| Utah | 18 | 2 | 1 | 21 | 1,991 | 163 | 2,154 | |||||||||||||||||||
| Colorado | 16 | 5 | 1 | 22 | 1,588 | 725 | 2,313 | |||||||||||||||||||
| Washington | 13 | 1 | — | 14 | 1,227 | 98 | 1,325 | |||||||||||||||||||
| Idaho | 11 | — | 1 | 12 | 998 | 21 | 1,019 | |||||||||||||||||||
| Nebraska | 4 | 1 | 2 | 7 | 413 | 305 | 718 | |||||||||||||||||||
| Kansas | — | — | 7 | 7 | 570 | 213 | 783 | |||||||||||||||||||
| Iowa | 4 | — | 2 | 6 | 368 | 31 | 399 | |||||||||||||||||||
| South Carolina | 7 | — | — | 7 | 866 | — | 866 | |||||||||||||||||||
| Nevada | 2 | — | — | 2 | 358 | — | 358 | |||||||||||||||||||
| 234 | 11 | 26 | 271 | 28,130 | 3,021 | 31,151 | ||||||||||||||||||||
Real Estate Properties — As of December 31, 2022, we owned 108 real estate properties in Arizona, California, Colorado, Idaho, Kansas, Nebraska, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin, which include 79 of the 271 facilities that we operate and manage. Of our 108 real estate properties, 29 senior living operations are leased to and operated by Pennant. One senior living operation leased by Pennant is located on the same real estate property as a skilled nursing facility that we own and operate. We further own the real estate property of our Service Center location and continue to lease a portion of the office space to third-party tenants. Our Standard Bearer segment reflects the results of operations for 103 of the 108 owned real estate properties.
The following table provides summary information regarding the location of our owned real estate properties as of December 31, 2022:
Owned and Operated by Ensign(1) | Owned and Leased to Pennant(1) | Service Center | Total Properties(1) | ||||||||||||||||||||
| California | 11 | 2 | 1 | 14 | |||||||||||||||||||
Texas(1) | 21 | 6 | — | 26 | |||||||||||||||||||
| Arizona | 13 | 1 | — | 14 | |||||||||||||||||||
| Wisconsin | 2 | 19 | — | 21 | |||||||||||||||||||
| Utah | 7 | — | — | 7 | |||||||||||||||||||
| Colorado | 7 | — | — | 7 | |||||||||||||||||||
| Washington | 2 | — | — | 2 | |||||||||||||||||||
| Idaho | 5 | — | — | 5 | |||||||||||||||||||
| Nebraska | 2 | — | — | 2 | |||||||||||||||||||
| Kansas | 4 | — | — | 4 | |||||||||||||||||||
| South Carolina | 5 | — | — | 5 | |||||||||||||||||||
| Nevada | — | 1 | — | 1 | |||||||||||||||||||
| 79 | 29 | 1 | 108 | ||||||||||||||||||||
(1) One senior living operation in Texas, which is owned by Ensign and leased to Pennant is located on the same real estate property as a skilled nursing facility that we own and operate. In this situation, the senior living operation is included in the total under "Owned and Leased to Pennant" and the skilled nursing operation is included in the total under "Owned and Operated by Ensign", however, the amount reflected under "Total Properties" only recognizes the operation as a single property.
64
Item 3. LEGAL PROCEEDINGS
Regulatory Matters — Laws and regulations governing Medicare and Medicaid programs are complex and subject to review and interpretation. Compliance with such laws and regulations is evaluated regularly, the results of which can be subject to future governmental review and interpretation, and can include significant regulatory action with fines, penalties, and exclusion from certain governmental programs. Included in these laws and regulations are rules requiring vaccination of employees and HIPAA, the terms of which require healthcare providers (among other things) to safeguard the privacy and security of certain patient protected health information.
Cost-Containment Measures — Both government and private pay sources have instituted cost-containment measures designed to limit payments made to providers of healthcare services, and there can be no assurance that future measures designed to limit payments made to providers will not adversely affect us.
Indemnities — From time to time, we enter into certain types of contracts that contingently require us to indemnify parties against third-party claims. These contracts primarily include (i) certain real estate leases, under which we may be required to indemnify property owners or prior facility operators for post-transfer environmental or other liabilities and other claims arising from our use of the applicable premises, (ii) operations transfer agreements, in which we agree to indemnify past operators of facilities we acquire against certain liabilities arising from the transfer of the operation and/or the operation thereof after the transfer to the Company's independent operating subsidiary, (iii) certain lending agreements, under which we may be required to indemnify the lender against various claims and liabilities, and (iv) certain agreements with our officers, directors and others, under which we may be required to indemnify such persons for liabilities arising out of the nature of their relationship to the Company. The terms of such obligations vary by contract and, in most instances, do not expressly state or include a specific or maximum dollar amount. Generally, amounts under these contracts cannot be reasonably estimated until a specific claim is asserted. Consequently, because no claims have been asserted, no liabilities have been recorded for these obligations on our balance sheets for any of the periods presented.
In connection with the spin-off transaction in 2019, certain landlords required, in exchange for their consent to the transaction, that our lease guarantees remain in place for a certain period of time following the spin-off. These guarantees could result in significant additional liabilities and obligations for us if Pennant were to default on their obligations under their leases with respect to these properties.
U.S. Department of Justice Civil Investigative Demand — On May 31, 2018, we received a CID from the U.S. Department of Justice stating that it was investigating to determine whether there had been a violation of the False Claims Act and/or the Anti-Kickback Statute with respect to the relationships between certain of our independently operated skilled nursing facilities and persons who serve or have served as medical directors, advisory board participants or other potential referral sources. The CID covered the period from October 3, 2013 through 2018, and was limited in scope to ten of our Southern California independent operating entities. In October 2018, the Department of Justice made an additional request for information covering the period of January 1, 2011 through 2018, relating to the same topic. As a general matter, our independent operating entities have established and maintain policies and procedures to promote compliance with the False Claims Act, the Anti-Kickback Statute, and other applicable regulatory requirements. We have fully cooperated with the U.S. Department of Justice and promptly responded to its requests for information; in April 2020, we were advised that the U.S. Department of Justice declined to intervene in any subsequent action filed by a relator in connection with the subject matter of this investigation.
Litigation — We and our independent operating entities are party to various legal actions and administrative proceedings, and are subject to various claims arising in the ordinary course of business, including claims that services provided to patients by our independent operating entities have resulted in injury or death, and claims related to employment and commercial matters. Although we intend to vigorously defend against these claims, there can be no assurance that the outcomes of these matters will not have a material adverse effect on operational results and financial condition. In certain states in which we have or have had independent operating entities, insurance coverage for the risk of punitive damages arising from general and professional liability litigation may not be available due to state law and/or public policy prohibitions. There can be no assurance that our independent operating entities will not be liable for punitive damages awarded in litigation arising in states for which punitive damage insurance coverage is not available.
65
The skilled nursing and post-acute care industry is heavily regulated. As such, we and our independent operating subsidiaries are continuously subject to state and federal regulatory scrutiny, supervision and control in the ordinary course of business. Such regulatory scrutiny often includes inquiries, investigations, examinations, audits, site visits and surveys, some of which are non-routine. In addition to being subject to direct regulatory oversight from state and federal agencies, the skilled nursing and post-acute care industry is also subject to regulatory requirements which could result in civil, administrative or criminal fines, penalties or restitutionary relief, and reimbursement; authorities could also seek the suspension or exclusion of the provider or individual from participation in their programs. We believe that there has been, and will continue to be, an increase in governmental investigations of LTC providers, particularly in the area of Medicare/Medicaid false claims, as well as an increase in enforcement actions resulting from these investigations. Adverse determinations in legal proceedings or governmental investigations, whether currently asserted or arising in the future, could have a material adverse effect on our financial position, results of operations, and cash flows.
Additionally, and in 2020, the U.S. House of Representatives Select Subcommittee on the Coronavirus Crisis launched a nation-wide investigation into the COVID-19 pandemic, which included the impact of the coronavirus on residents and employees in nursing homes. In June 2020, we and our independent operating subsidiaries received a document and information request from the House Select Subcommittee. We and our independent operating subsidiaries have cooperated in responding to this inquiry. In July 2022 and thereafter, we and our independent operating subsidiaries received follow up requests for additional documents and information. We and our independent operating subsidiaries have responded to these requests, and continued to cooperate with the House Select Subcommittee in connection with its investigation. On December 9, 2022, the House Select Subcommittee issued its final report summarizing its investigation and related recommendations designed "to strengthen the nation's ability to prevent and respond to public health and economic emergencies." According to the information provided by the House Select Subcommittee, the issuance of this report was the House Select Subcommittee's final official act.
In addition to the potential lawsuits and claims described above, we and our independent operating subsidiaries are also subject to potential lawsuits under the Federal False Claims Act and comparable state laws alleging submission of fraudulent claims for services to any healthcare program (such as Medicare or Medicaid) or other payor. A violation may provide the basis for exclusion from Federally funded healthcare programs. Such exclusions could have a correlative negative impact on our financial performance. Under the qui tam or "whistleblower" provisions of the False Claims Act, a private individual with knowledge of fraud or potential fraud may bring a claim on behalf of the Federal Government and receive a percentage of the Federal Government's recovery. Due to these whistleblower incentives, qui tam lawsuits have become more frequent. For example, and despite the decision of the U.S. Department of Justice to decline to participate in litigation based on the subject matter of its previously issued Civil Investigative Demand, the involved qui tam relator is continuing on with the lawsuit and pursuing claims that one or more of the Company's independent operating entities have allegedly violated the False Claims Act and/or the AKS.
In addition to the Federal False Claims Act, some states, including California, Arizona and Texas, have enacted similar whistleblower and false claims laws and regulations. Further, the Deficit Reduction Act of 2005 created incentives for states to enact anti-fraud legislation modeled on the Federal False Claims Act. As such, we and our independent operating subsidiaries could face increased scrutiny, potential liability, and legal expenses and costs based on claims under state false claims acts in markets where our independent operating subsidiaries do business.
In May 2009, Congress passed the FERA which made significant changes to the Federal False Claims Act (FCA) and expanded the types of activities subject to prosecution and whistleblower liability. Following changes by FERA, health care providers face significant penalties for the knowing retention of government overpayments, even if no false claim was involved. Health care providers can now be liable for knowingly and improperly avoiding or decreasing an obligation to pay money or property to the government. This includes the retention of any government overpayment. The government can argue, therefore, that an FCA violation can occur without any affirmative fraudulent action or statement, as long as the action or statement is knowingly improper. In addition, FERA extended protections against retaliation for whistleblowers, including protections not only for employees, but also contractors and agents. Thus, an employment relationship is generally not required in order to qualify for protection against retaliation for whistleblowing.
Healthcare litigation (including class action litigation) is common and is filed based upon a wide variety of claims and theories, and our independent operating entities are routinely subjected to varying types of claims, including class action "staffing" suits where the allegation is understaffing at the facility level. These class-action “staffing” suits have the potential to result in large jury verdicts and settlements. We expect the plaintiffs' bar to continue to be aggressive in their pursuit of these staffing and similar claims.
66
We and our independent operating subsidiaries have been, and continue to be, subject to claims, findings and legal actions that arise in the ordinary course of the various businesses, including healthcare and non-healthcare services. These claims include, but are not limited to potential claims related to patient care and treatment (professional negligence claims) as well as employment related claims. In addition, we and our independent operating subsidiaries, and others in the industry, are subject to claims and lawsuits in connection with COVID-19 and facility preparation for and/or response to the COVID-19 pandemic. While we have been able to settle or otherwise resolve these types of claims without an ongoing material adverse effect on our business, a significant increase in the number of these claims, or an increase in the amounts owing should plaintiffs be successful in their prosecution of future claims, could materially adversely affect the Company’s business, financial condition, results of operations and cash flows. In addition, these claims could impact our ability to procure insurance to cover our exposure related to the various services provided by our independent operating subsidiaries to their residents, customers and patients.
Claims and suits, including class actions, continue to be filed against our independent operating subsidiaries and other companies in the post-acute care industry. We and our independent operating entities have been subjected to, and/or are currently involved in, class action litigation alleging violations (alone or in combination) of state and federal wage and hour law as related to the alleged failure to pay wages, to timely provide and authorize meal and rest breaks, and other such similar causes of action. We do not believe that the ultimate resolution of these actions will have a material adverse effect on our business, cash flows, financial condition or results of operations.
Medicare Revenue Recoupments — We and our independent operating subsidiaries are subject to regulatory reviews relating to the provision of Medicare services, billings and potential overpayments resulting from reviews conducted via RAC, Program Safeguard Contractors, and Medicaid Integrity Contractors (collectively referred to as Reviews). For several months during the COVID-19 pandemic, CMS suspended its Targeted Probe and Educate Program. Beginning in August 2020, CMS resumed Targeted Probe and Educate Program activity. If an operation fails a Review and/or subsequent Reviews, the operation could then be subject to extended review or an extrapolation of the identified error rate to billings in the same time period. We anticipate that these Reviews could increase in frequency in the future. As of December 31, 2022 and since, 34 of our independent operating subsidiaries had Reviews scheduled, on appeal, or in a dispute resolution process.
Item 4. MINE SAFETY DISCLOSURES
None.
PART II.
Item 5. MARKET FOR REGISTRANT'S COMMON EQUITY, RELATED STOCKHOLDER MATTERS AND ISSUER PURCHASES OF EQUITY SECURITIES
Market Information
Our common stock has been traded under the symbol “ENSG” on the NASDAQ Global Select Market since our initial public offering on November 8, 2007. Prior to that time, there was no public market for our common stock. As of January 30, 2023, there were approximately 297 holders of record of our common stock.
Notwithstanding anything to the contrary set forth in any of our filings under the Securities Act or the Exchange Act that might incorporate future filings, including the Annual Report on Form 10-K, in whole or in part, the Stock Performance Graph and supporting data which follows shall not be deemed to be incorporated by reference into any such filings except to the extent that we specifically incorporate any such information into any such future filings.
The graph below shows the cumulative total stockholder return of investment of $100 (and the reinvestment of any dividends thereafter) on December 31, 2017 in (i) our common stock, (ii) the Skilled Nursing Facilities Peer Group 1 and (iii) the NASDAQ Market Index. Our stock price performance shown in the graph below is not indicative of future stock price performance.
On October 1, 2019, Ensign completed the spin-off of The Pennant Group, Inc. (Pennant) with the pro rata distribution of 1.18 shares of Pennant’s common stock for every share of Ensign’s common stock to our stockholders, pursuant to which Pennant became an independent company. Pennant's stock traded at $6.15 at opening price on the first day of trading and closed at $15.09. Ensign's stock price was reduced by the same value on the same day. For the purpose of this graph, the effect of the final separation of Pennant is reflected in the cumulative total return of Ensign Common Stock as a reinvested dividend.
67
COMPARISON OF 60 MONTH CUMULATIVE TOTAL RETURN*
Among Ensign Group, the NASDAQ Composite Index and Our Peer Group
December 2022
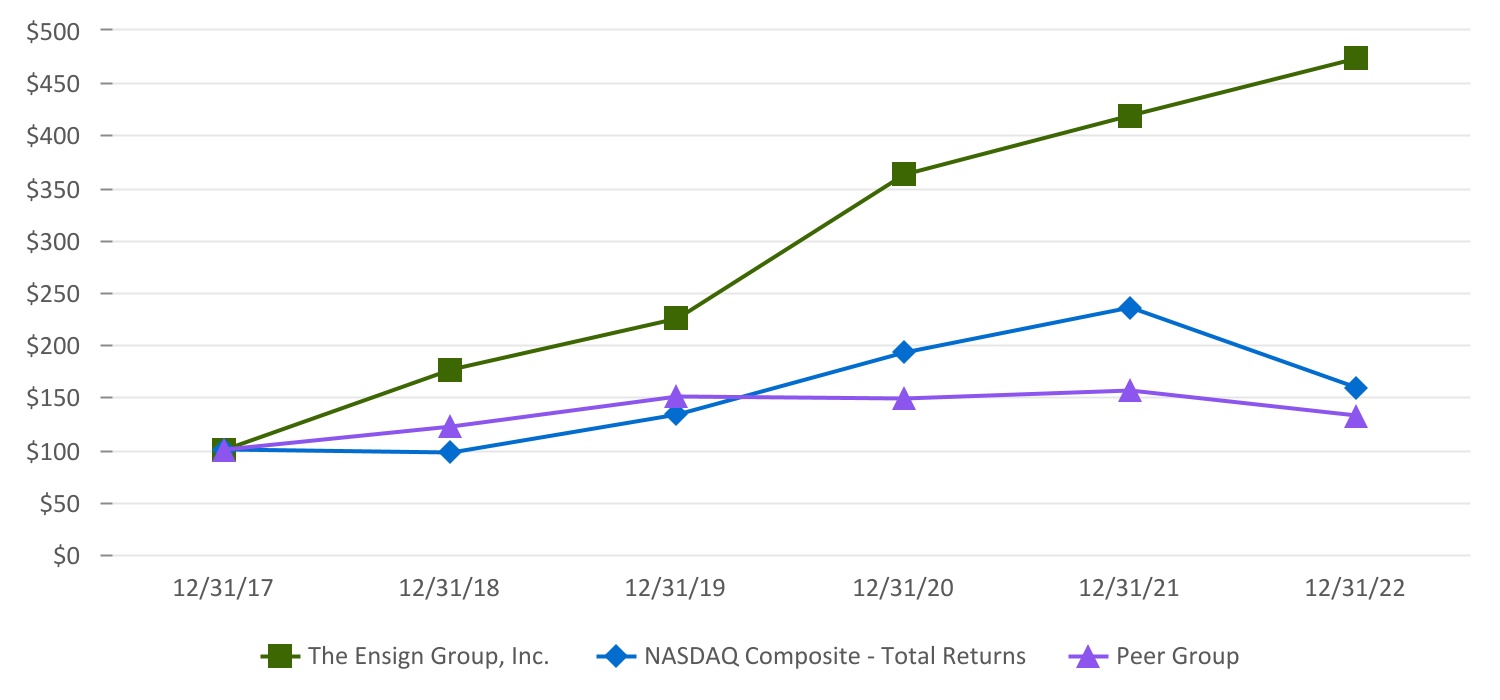
*Assumes $100 invested on December 31, 2017 in stock in index, including reinvestment of dividends.
Fiscal year ended December 31.
| December 31, | ||||||||||||||||||||||||||||||||||||||
| 2017 | 2018 | 2019 | 2020 | 2021 | 2022 | |||||||||||||||||||||||||||||||||
The Ensign Group, Inc.(2) | $ | 100.00 | $ | 175.65 | $ | 224.56 | $ | 362.38 | $ | 418.24 | $ | 472.47 | ||||||||||||||||||||||||||
| NASDAQ Market Index | 100.00 | 97.16 | 132.81 | 192.47 | 235.15 | 158.65 | ||||||||||||||||||||||||||||||||
Peer Group(1) | 100.00 | 121.42 | 150.55 | 148.58 | 155.55 | 132.19 | ||||||||||||||||||||||||||||||||
(1) The current composition of our Peer Group is as follows: Amedysis, Inc., CareTrust REIT Inc., Encompass Healthcare Corp., LTC Properties, Inc., National Healthcare Corporation, National Health Investors, Inc., Omega Healthcare Investors, Inc., Select Medical Holdings Corp. and Welltower Inc.
(2) The value displayed only incorporates the value of The Ensign Group, Inc. stock and does not incorporate the value shareholders received in connection with our spin-offs of CareTrust REIT Inc. and The Pennant Group, Inc.
Dividend Policy
We do not have a formal dividend policy, but we currently intend to continue to pay regular quarterly dividends to the holders of our common stock. We have been a dividend-paying company since 2002 and have increased our dividend every year for the last 20 years.
Issuer Repurchases of Equity Securities
Stock Repurchase Programs — On July 28, 2022, the Board of Directors approved a stock repurchase program pursuant to which we could repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from August 2, 2022. Under this program, we are authorized to repurchase our issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. We did not purchase any shares pursuant to this stock repurchase program in the year ended December 31, 2022. The share repurchase program does not obligate us to acquire any specific number of shares.
68
On February 9, 2022, the Board of Directors approved a stock repurchase program pursuant to which we could repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from February 10, 2022. Under this program, we were authorized to repurchase our issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. During the second quarter of 2022, we repurchased 0.3 million shares of our common stock for $20.0 million. This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
On October 21, 2021, the Board of Directors approved a stock repurchase program pursuant to which we could repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from October 29, 2021. Under this program, we were authorized to repurchase our issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. During the first quarter of 2022, we repurchased 0.1 million shares of our common stock for $9.9 million. During the fourth quarter of 2021, we repurchased 0.1 million shares of our common stock for $10.1 million. This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
A summary of the repurchase activity for the year ended December 31, 2022 is as follows (dollars in millions, except per share amounts):
| Period | Total Number of Shares Repurchased | Average Price Per Share | Total Number of Shares Purchased as Part of Publicly Announced Plans or Programs | Approximate Dollar Value of Shares that May Yet Be Purchased Under the Plans or Programs | ||||||||||||||||||||||
First quarter of 2022(1) | 133,328 | $ | 74.09 | 133,328 | $ | 20.0 | ||||||||||||||||||||
Second quarter of 2022(2) | 270,720 | 73.85 | 270,720 | — | ||||||||||||||||||||||
| Third quarter of 2022 | — | — | — | 20.0 | ||||||||||||||||||||||
| October 1 to October 31, 2022 | — | — | — | 20.0 | ||||||||||||||||||||||
| November 1 to November 30, 2022 | — | — | — | 20.0 | ||||||||||||||||||||||
| December 1 to December 31, 2022 | — | $ | — | — | $ | 20.0 | ||||||||||||||||||||
(1) These purchases were effectuated through a Rule 10b5-1 trading plan adopted by the Company on October 21, 2021.
(2) These purchases were effectuated through a Rule 10b5-1 trading plan adopted by the Company on February 9, 2022.
Item 6. [RESERVED]
Item 7. MANAGEMENT'S DISCUSSION AND ANALYSIS OF FINANCIAL CONDITION AND RESULTS OF OPERATIONS
The following discussion should be read in conjunction with the consolidated financial statements and accompanying notes, which appear elsewhere in this Annual Report on Form 10-K. This discussion contains forward-looking statements that involve risks and uncertainties. Our actual results could differ materially from those anticipated in these forward-looking statements as a result of various factors, including those discussed below and elsewhere in this Annual Report on Form 10-K. See Part I. Item 1A. Risk Factors and Cautionary Note Regarding Forward-Looking Statements.
For discussion of 2020 items and year-over-year comparisons between 2021 and 2020 that are not included in this 2022 Form 10-K, refer to “Item 7. – Management’s Discussion and Analysis of Financial Condition and Results of Operations” found in our Form 10-K for the year ended December 31, 2021, that was filed with the Securities and Exchange Commission on February 9, 2022.
69
Overview
We are a provider of health care services across the post-acute care continuum, engaged in the operation, ownership, acquisition, development and leasing of skilled nursing, senior living and other healthcare related properties and other ancillary businesses located in Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin. Our operating subsidiaries, each of which strives to be the operation of choice in the community it serves, provide a broad spectrum of skilled nursing, senior living and other ancillary services. As of December 31, 2022, we offered skilled nursing, senior living and rehabilitative care services through 271 skilled nursing and senior living facilities. Of the 271 facilities, we operated 192 facilities under long-term lease arrangements and have options to purchase 11 of those facilities. Our real estate portfolio includes 108 owned real estate properties, which included 79 facilities operated and managed by us, 29 senior living operations leased to and operated by The Pennant Group, Inc., or Pennant, as part of the spin-off transaction that occurred in October 2019, and the Service Center location. Of the 29 real estate operations leased to Pennant, one senior living operation is located on the same real estate property as a skilled nursing facility that we own and operate.
Ensign is a holding company with no direct operating assets, employees or revenues. Our operating subsidiaries are operated by separate, independent entities, each of which has its own management, employees and assets. In addition, certain of our wholly-owned subsidiaries, referred to collectively as the Service Center, provide centralized accounting, payroll, human resources, information technology, legal, risk management and other centralized services to the other operating subsidiaries through contractual relationships with such subsidiaries. We also have a wholly-owned captive insurance subsidiary that provides some claims-made coverage to our operating subsidiaries for general and professional liability, as well as coverage for certain workers’ compensation insurance liabilities and our captive real estate trust owns and operates our real estate portfolio. Our captive real estate investment trust, Standard Bearer, owns and manages our real estate business. References herein to the consolidated “Company” and “its” assets and activities, as well as the use of the terms “we,” “us,” “our” and similar terms in this Annual Report, are not meant to imply, nor should they be construed as meaning, that The Ensign Group, Inc. has direct operating assets, employees or revenue, or that any of the subsidiaries are operated by The Ensign Group.
Recent Activities
Operational Update — In 2022, the public health emergency (PHE) was extended several times and was most recently extended through April 11, 2023. On January 30, 2023, the Biden Administration announced its plan to extend the PHE for a final time to May 11, 2023. Our primary focus continues to be the health and safety of our patients, residents, employees and their respective families. We continue to implement measures necessary to provide the safest possible environment within our sites of service, taking into consideration the vulnerable nature of our patients and the unique exposure risks of our staff.
We continue to execute on key initiatives to rebuild occupancy lost due to the pandemic. During the year, our combined Same Facilities and Transitioning Facilities occupancy increased by 2.9% compared to 2021. The improvements in occupancy were due to our operations developing innovative approaches to confront the occupancy declines, including strategic partnerships with upstream and downstream continuum partners and increasing clinical competencies to treat high-acuity patients, including those that are COVID-19 positive. We believe our operations will continue to gain additional market share as a result of relationships with acute care providers and other health care partners.
During the year ended December 31, 2022 and 2021, we recognized $81.8 million and $75.2 million, respectively, of state relief funding as revenue, including FMAP.
The CARES Act also provides for deferred payment of the employer portion of social security taxes through the end of 2020, with approximately 50% of the deferred amount paid by December 31, 2021 and the remaining 50% by December 31, 2022. See Note 3, COVID-19 Update in the Notes to the Consolidated Financial Statements.
Captive Real Estate Investment Trust — In January of 2022, we formed Standard Bearer Healthcare REIT, Inc. or Standard Bearer, a captive REIT. Standard Bearer is a holding company with subsidiaries that own most of our real estate portfolio. We expect the REIT structure will allow us to better demonstrate the growing value of our owned real estate and provides us with an efficient vehicle for future acquisitions of properties that could be operated by Ensign affiliates or other third parties. We believe this structure will give us new pathways to growth with transactions we would not have considered in the past. Standard Bearer intends to qualify and elects to be taxed as a REIT, for U.S. federal income tax purposes, commencing with its taxable year ended December 31, 2022.
70
During the year ended December 31, 2022, we acquired the real estate of ten skilled nursing facilities, all of which were leased to certain of our operating subsidiaries through the Standard Bearer Master Leases for a purchase price of $84.7 million. Of the ten, three were previously operated and managed by us. The resulting real estate portfolio in Standard Bearer consists of a select 103 of our 108 owned real estate properties. Of the 103 owned real estate properties in Standard Bearer, 75 facilities are operated by Ensign operating subsidiaries and 29 facilities are leased to and operated by Pennant. Of the 29 real estate operations leased to Pennant, one senior living operation is located on the same real estate property as a skilled nursing facility that we own and operate. In addition, as we expand our real estate portfolio through our acquisition strategy, we anticipate that the acquired real estate will be included in Standard Bearer.
As of December 31, 2022, the fair value of Standard Bearer's real estate portfolio is approximately $1.1 billion. The fair value was determined by a third party independent valuation specialist and incorporated each property's rental income, capitalization rate, rental yield rate and discount rate.
As part of the formation of Standard Bearer, certain of our operating subsidiaries and the Standard Bearer subsidiaries entered into five "triple-net" master lease agreements (collectively, the Standard Bearer Master Leases). Total annual rental income under the Standard Bearer Master Lease is approximately $62.5 million.
Standard Bearer has no employees. Personnel and services provided to Standard Bearer by the Service Center are pursuant to the management agreement between Standard Bearer and the Service Center. The management agreement provides for a base management fee and an incentive management fee, payable in cash, among other terms. The base management fee for each applicable period is equal to 5.0% of the total revenue of Standard Bearer. The incentive management fee is equal to 5.0% of funds from operations (FFO) and is capped at 1.0% of total revenue. In addition, operating expenses incurred by the Service Center on Standard Bearer's behalf, which includes the cost of legal, tax, consulting, accounting and other similar services rendered by the Service Center, its advisers or other third parties, are reimbursed by Standard Bearer. During the year ended December 31, 2022, the Service Center management fee was $4.4 million, which represents 6% of total Standard Bearer rental revenue.
Standard Bearer will obtain its funding through various sources including operating cash flows, access to debt arrangements and intercompany loans. The intercompany debt arrangements include mortgage loans and the Revolving Credit Facility to fund acquisitions and working capital needs. As part of the Amended Credit Agreement discussed in Note 16, Debt, the interest rates applicable to loans under the Revolving Credit Facility were amended, such that the rates are, at the Company's option, equal to either a base rate plus a margin ranging from 0.25% to 1.25% per annum or SOFR plus a margin range from 1.25% to 2.25% per annum.
During the year ended December 31, 2022, Standard Bearer established shareholders of its preferred shares through contributions of cash of $0.1 million. These preferred shares were fully vested at the time of the contributions by the shareholders. In addition, as part of the formation of Standard Bearer in January of 2022, we established the Standard Bearer Healthcare REIT, Inc. 2022 Omnibus Incentive Plan (Standard Bearer Equity Plan). In 2022, Standard Bearer sold fully vested common shares from the Standard Bearer Equity Plan to shareholders for cash of $6.5 million. We did not grant any stock options nor restricted shares during the year ended December 31, 2022.
During the year ended December 31, 2022, Standard Bearer met the requirement to distribute to its shareholders at least 90% of its annual taxable income through a declaration and payment of cash dividends totaling $30.4 million. Of that amount, $30.1 million was paid in the form of a distribution to the Company and $0.3 million was paid in the form of a distribution to noncontrolling interests.
Revolving Credit Facility Amendment — On April 8, 2022, we entered into the Second Amendment to the Third Amended and Restated Credit Facility (such agreement, the Amended Credit Agreement, and the revolving credit facility thereunder, the Revolving Credit Facility), which increased the Revolving Credit Facility by $250.0 million to an aggregate principal amount of up to $600.0 million. Pursuant to the Amended Credit Agreement, the Company transitioned from the London Interbank Offered Rate (LIBOR) to the Secured Overnight Financing Rate (SOFR) as the applicable reference rate for borrowings under the Revolving Credit Facility. The maturity date of the Amended Credit Facility is April 8, 2027. Borrowings are supported by a lending consortium arranged by Truist Securities (Truist). The interest rates applicable to loans under the Revolving Credit Facility are, at our option, equal to either a base rate plus a margin ranging from 0.25% to 1.25% per annum or SOFR plus a margin range from 1.25% to 2.25% per annum, based on the Consolidated Total Net Debt to Consolidated EBITDA ratio (as defined in the Amended Credit Agreement). In addition, we will pay a commitment fee on the unused portion of the commitments, which will range from 0.20% to 0.40% per annum, depending on the Consolidated Total Net Debt to Consolidated EBITDA ratio. As part of the amendment, deferred financing costs of $0.6 million were written off and additional deferred financing costs of $3.2 million were capitalized during the year ended December 31, 2022.
71
Common Stock Repurchase Program — On July 28, 2022, the Board of Directors approved a stock repurchase program pursuant to which we may repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from August 2, 2022. We did not purchase any shares pursuant to this stock repurchase program in the year ended December 31, 2022. On February 9, 2022, the Board of Directors approved a stock repurchase program pursuant to which we could repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from February 10, 2022. In the second quarter of 2022, we repurchased 0.3 million shares of our common stock for $20.0 million. This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
We manage the fiscal aspects of our business by monitoring key performance indicators that affect our financial performance. Revenue associated with these metrics is generated based on contractually agreed-upon amounts or rate, excluding the estimates of variable consideration under the revenue recognition standard, Financial Accounting Standards Board (FASB) Accounting Standards Codification (ASC) Topic 606. These indicators and their definitions include the following:
Skilled Services
•Routine revenue — Routine revenue is generated by the contracted daily rate charged for all contractually inclusive skilled nursing services. The inclusion of therapy and other ancillary treatments varies by payor source and by contract. Services provided outside of the routine contractual agreement are recorded separately as ancillary revenue, including Medicare Part B therapy services, and are not included in the routine revenue definition.
•Skilled revenue - The amount of routine revenue generated from patients in the skilled nursing facilities who are receiving higher levels of care under Medicare, managed care, Medicaid, or other skilled reimbursement programs. The other skilled patients who are included in this population represent very high acuity patients who are receiving high levels of nursing and ancillary services which are reimbursed by payors other than Medicare or managed care. Skilled revenue excludes any revenue generated from our senior living services.
•Skilled mix — The amount of our skilled revenue as a percentage of our total skilled nursing routine revenue. Skilled mix (in days) represents the number of days our Medicare, managed care, or other skilled patients are receiving skilled nursing services at the skilled nursing facilities divided by the total number of days patients from all payor sources are receiving skilled nursing services at the skilled nursing facilities for any given period.
•Average daily rates — The routine revenue by payor source for a period at the skilled nursing facilities divided by actual patient days for that revenue source for that given period. These rates exclude additional state relief funding, which includes payments we recognized as part of The Family First Coronavirus Response Act.
•Occupancy percentage (operational beds) — The total number of patients occupying a bed in a skilled nursing facility as a percentage of the beds in a facility which are available for occupancy during the measurement period.
•Number of facilities and operational beds — The total number of skilled nursing facilities that we own or operate and the total number of operational beds associated with these facilities.
Skilled Mix — Like most skilled nursing providers, we measure both patient days and revenue by payor. Medicare, managed care and other skilled patients, whom we refer to as high acuity patients, typically require a higher level of skilled nursing and rehabilitative care. Accordingly, Medicare and managed care reimbursement rates are typically higher than from other payors. In most states, Medicaid reimbursement rates are generally the lowest of all payor types. Changes in the payor mix can significantly affect our revenue and profitability.
The following table summarizes our overall skilled mix from our skilled nursing services for the periods indicated as a percentage of our total skilled nursing routine revenue and as a percentage of total skilled nursing patient days:
| Year Ended December 31, | |||||||||||
| Skilled Mix: | 2022 | 2021 | |||||||||
| Days | 31.8 | % | 31.7 | % | |||||||
| Revenue | 52.0 | % | 52.3 | % | |||||||
72
Occupancy — We define occupancy derived from our skilled services as the ratio of actual patient days (one patient day equals one patient occupying one bed for one day) during any measurement period to the number of beds in facilities which are available for occupancy during the measurement period. The number of beds in a skilled nursing facility that are actually operational and available for occupancy may be less than the total official licensed bed capacity. This sometimes occurs due to the permanent dedication of bed space to alternative purposes, such as enhanced therapy treatment space or other desirable uses calculated to improve service offerings and/or operational efficiencies in a facility. In some cases, three- and four-bed wards have been reduced to two-bed rooms for resident comfort, and larger wards have been reduced to conform to changes in Medicare requirements. These beds are seldom expected to be placed back into service. We believe that reporting occupancy based on operational beds is consistent with industry practices and provides a more useful measure of actual occupancy performance from period to period.
The following table summarizes our overall occupancy statistics for skilled nursing operations for the periods indicated:
| Year Ended December 31, | |||||||||||
| Occupancy for skilled services: | 2022 | 2021 | |||||||||
| Operational beds at end of period | 28,130 | 25,032 | |||||||||
| Available patient days | 9,614,460 | 8,895,949 | |||||||||
| Actual patient days | 7,243,781 | 6,478,810 | |||||||||
| Occupancy percentage (based on operational beds) | 75.3 | % | 72.8 | % | |||||||
Segments
We have two reportable segments: (1) skilled services, which includes the operation of skilled nursing facilities and rehabilitation therapy services and (2) Standard Bearer, which is comprised of select properties owned by us through our captive REIT and leased to skilled nursing and senior living operations, including our own operating subsidiaries and third party operators.
We also reported an “all other” category that includes operating results from our senior living operations, mobile diagnostics, transportation, other real estate and other ancillary operations. These businesses are neither significant individually, nor in aggregate and therefore do not constitute a reportable segment. Our Chief Executive Officer, who is our chief operating decision maker, or CODM, reviews financial information at the operating segment level.
Within our skilled nursing operations, we generate revenue from Medicaid, private pay, managed care and Medicare payors. We believe that our skilled mix, which we define as the number of days Medicare, managed care and other skilled patients are receiving services at our skilled nursing operations divided by the total number of days patients are receiving services at our skilled nursing operations, from all payor sources (less days from senior living services) for any given period, is an important indicator of our success in attracting high-acuity patients because it represents the percentage of our patients who are reimbursed by Medicare, managed care and other skilled payors, for whom we receive higher reimbursement rates.
We are participating in supplemental payment programs in various states that provide supplemental Medicaid payments for skilled nursing facilities that are licensed to non-state government-owned entities such as city and county hospital districts. Numerous operating subsidiaries entered into transactions with various hospital districts providing for the transfer of the licenses for those skilled nursing facilities to the hospital districts. Each affected operating subsidiary agreement between the hospital district and our subsidiary is terminable by either party to fully restore the prior license status.
73
Standard Bearer
We generate rental revenue primarily by leasing post-acute care properties we acquired to healthcare operators under triple-net lease arrangements, whereby the tenant is solely responsible for the costs related to the property, including property taxes, insurance and maintenance and repair costs, subject to certain exceptions. As of December 31, 2022, our real estate portfolio within Standard Bearer is comprised of 103 real estate properties. Of these properties, 75 are leased to affiliated skilled nursing facilities wholly-owned and managed by us and 29 are leased to senior living operations wholly-owned and managed by Pennant. Of the 29 real estate operations leased to Pennant, one senior living operation is located on the same real estate property as a skilled nursing facility that we own and operate. During the year ended December 31, 2022, we generated rental revenues of $72.9 million, of which $58.0 million was derived from affiliated wholly-owned healthcare operators, and therefore eliminated in consolidation.
Other
Within our senior living operations, we generate revenue primarily from private pay sources, with a portion earned from Medicaid payors or through other state-specific programs. In addition, we hold majority membership interests in certain of our other ancillary operations. Payment for these services varies and is based upon the service provided. The payment is adjusted for an inability to obtain appropriate billing documentation or authorizations acceptable to the payor and other reasons unrelated to credit risk.
Primary Components of Expense
Cost of Services (exclusive of rent and depreciation and amortization shown separately) — Our cost of services represents the costs of operating our operating subsidiaries, which primarily consists of payroll and related benefits, supplies, purchased services, and ancillary expenses such as the cost of pharmacy and therapy services provided to patients. Cost of services also includes the cost of general and professional liability insurance, rent expenses related to leasing our operational facilities that are not included in facility rent - cost of services, and other general cost of services with respect to our operations.
Facility Rent - Cost of Services — Rent - cost of services consists solely of base minimum rent amounts payable under lease agreements to third-party real estate owners. Our operating subsidiaries lease and operate but do not own the underlying real estate and these amounts do not include taxes, insurance, impounds, capital reserves or other charges payable under the applicable lease agreements. Expenses related to leasing our operations are included in cost of services.
General and Administrative Expense — General and administrative expense consists primarily of payroll and related benefits and travel expenses for our Service Center personnel, including training and other operational support. General and administrative expense also includes professional fees (including accounting and legal fees), costs relating to our information systems and stock-based compensation related to our Service Center employees.
Depreciation and Amortization — Property and equipment are recorded at their original historical cost. Depreciation is computed using the straight-line method over the estimated useful lives of the depreciable assets. The following is a summary of the depreciable lives of our depreciable assets:
| Buildings and improvements | Minimum of three years to a maximum of 59 years, generally 45 years | |||||||
| Leasehold improvements | Shorter of the lease term or estimated useful life, generally 5 to 15 years | |||||||
| Furniture and equipment | 3 to 10 years | |||||||
Critical Accounting Estimates
Our discussion and analysis of our financial condition and results of operations are based on our consolidated financial statements, which have been prepared in accordance with U.S. Generally Accepted Accounting Principles (GAAP). The preparation of these financial statements and related disclosures requires us to make judgments, estimates and assumptions that affect the reported amounts of assets and liabilities and disclosure of contingent assets and liabilities at the date of the financial statements and the reported amounts of revenue and expenses during the reporting period. We believe that the application of the following accounting policies, which are important to our financial position and results of operations, require significant judgments and estimates on the part of management. For a summary of our significant accounting policies, including the accounting policies discussed below, see Note 2, “Summary of Significant Accounting Policies” of the Notes to Consolidated Financial Statements.
74
Variable consideration within revenue recognition — Revenue recognized from healthcare services are adjusted for estimates of variable consideration to arrive at the transaction price. We determine the transaction price based on contractually agreed-upon amounts or rates, adjusted for estimates of variable consideration. We use the expected value method in determining the variable component that should be used to arrive at the transaction price, using contractual agreements and historical reimbursement experience within each payor type. The amount of variable consideration which is included in the transaction price may be constrained and is included in the net revenue only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will not occur in a future period. If actual amounts of consideration ultimately received differ from our estimates, we adjust these estimates, which would affect net service revenue in the period such variances become known.
Self-insurance for general and professional liability — The self-insured retention and deductible limits for general and professional liability for all states are self-insured through our wholly owned captive insurance subsidiary (the Captive Insurance), the related assets and liabilities of which are included in the accompanying consolidated balance sheets. Our general and professional liability as of the years ended December 31, 2022 and 2021 was $87.0 million and $69.7 million, respectively.
Our policy is to accrue amounts equal to the actuarially estimated costs to settle open claims of insureds, as well as an estimate of the cost of insured claims that have been incurred but not reported. We develop information about the size of the ultimate claims based on historical experience, current industry information and actuarial analysis, and evaluate the estimates for claim loss exposure on a quarterly basis. We use actuarial valuations to estimate the liability based on historical experience and industry information.
RESULTS OF OPERATIONS
We believe we exist to dignify and transform post-acute care. We set out a strategy to achieve our goal of ensuring our patients are receiving the best possible care through our ability to acquire, integrate and improve our operations. Our results serve as a strong indicator that our strategy is working and our transformation is underway. Since 2018, our total revenue increased $1.3 billion, or 72.4%, representing a 14.6% compound annual growth rate (CAGR) while our diluted GAAP earning per share (EPS) from continued operations grew by $2.86 from 2018 to $3.95, representing a 38.0% CAGR.
Our total revenue for the year ended December 31, 2022 increased $398.0 million, or 15.1%, while our diluted GAAP earning per share grew by 15.5%, from $3.42 to $3.95, compared to the year ended December 31, 2021. Over the past year, we have continued to make progress on targeted initiatives related to increasing occupancy and hiring and developing our people. Our combined Same Facilities and Transitioning Facilities occupancy increased by 2.9% compared to 2021. We saw a recovery in our census starting in the first quarter of 2021, which has continued throughout 2022. Despite the emergence of COVID-19 variants and subvariants throughout 2022, we continue to experience healthy growth in both revenue and operational earnings. We also added over 4,000 team members, or 16%, to our operating subsidiaries and the Service Center.
Our net revenue for the year ended December 31, 2022 continued to be impacted by COVID-19, with the continual evolution of COVID-19 variants and subvariants in 2022. Accordingly, we continued to receive state relief funding in selected states, which have been designed to provide additional funding to cover COVID-19 related expenses. For the year ended December 31, 2022, we recorded state relief revenue of $81.8 million, which directly offsets against COVID-19 related expenses we incurred in those states. See Recent Activities for further information.
Additionally, we continue to seek out opportunities to expand our operations and real estate, adding 29 new operations and ten real estate properties, three of which we previously operated, during the year ended December 31, 2022. We remain confident that our operating model will continue to allow each operator to form their own market-specific strategy and to adjust to the needs of their local medical communities, including methods for attracting new healthcare professionals into our workforce and retaining and developing existing staff. We are excited to be adding new operations in several geographies. These transitions will take time, particularly given the continued labor pressures, but with each new operation we are creating new opportunities for the next generation of leaders and look forward to working together to help each operation reach its enormous clinical and financial potential.
75
The following table sets forth details of operating results for our revenue, expenses and earnings, and their respective components, as a percentage of total revenue for the periods indicated:
| Year Ended December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| REVENUE: | |||||||||||
| Service revenue | 99.4 | % | 99.4 | % | |||||||
| Rental revenue | 0.6 | 0.6 | |||||||||
| TOTAL REVENUE | 100.0 | % | 100.0 | % | |||||||
| Expenses: | |||||||||||
| Cost of services | 77.8 | 76.9 | |||||||||
| Rent—cost of services | 5.1 | 5.3 | |||||||||
| General and administrative expense | 5.2 | 5.8 | |||||||||
| Depreciation and amortization | 2.1 | 2.1 | |||||||||
| TOTAL EXPENSES | 90.2 | 90.1 | |||||||||
| Income from operations | 9.8 | 9.9 | |||||||||
| Other income (expense): | |||||||||||
| Interest expense | (0.3) | (0.3) | |||||||||
| Other income | — | 0.2 | |||||||||
| Other expense, net | (0.3) | (0.1) | |||||||||
| Income before provision for income taxes | 9.5 | 9.8 | |||||||||
| Provision for income taxes | 2.1 | 2.3 | |||||||||
| NET INCOME | 7.4 | 7.5 | |||||||||
| Less: net income attributable to noncontrolling interests | — | 0.1 | |||||||||
| Net income attributable to The Ensign Group, Inc. | 7.4 | % | 7.4 | % | |||||||
| Year Ended December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
SEGMENT INCOME(1) | (In thousands) | ||||||||||
| Skilled services | $ | 408,732 | $ | 373,603 | |||||||
Standard Bearer(2) | 27,871 | 31,876 | |||||||||
| NON-GAAP FINANCIAL MEASURES: | |||||||||||
| PERFORMANCE METRICS | |||||||||||
| EBITDA | 359,209 | 313,377 | |||||||||
| Adjusted EBITDA | 383,570 | 336,572 | |||||||||
FFO for Standard Bearer | 49,484 | 49,434 | |||||||||
| VALUATION METRICS | |||||||||||
| Adjusted EBITDAR | $ | 536,619 | |||||||||
(1) Segment income represents operating results of the reportable segments excluding gain and loss on sale of assets, real estate insurance recoveries and losses, impairment charges and provision for income taxes. Included in segment income for Standard Bearer for the year ended December 31, 2022 are expenses for intercompany management fees between Standard Bearer and the Service Center and intercompany interest expense. Segment income is reconciled to the Consolidated Statement of Income in Note 8, Business Segments in Notes to Consolidated Financial Statements of this Annual Report on Form 10-K.
(2) Standard Bearer segment income includes rental revenue from Ensign affiliated tenants and related expenses.
76
The following discussion includes references to EBITDA, Adjusted EBITDA, Adjusted EBITDAR and Funds from Operations (FFO) which are non-GAAP financial measures (collectively, the Non-GAAP Financial Measures). Regulation G, Conditions for Use of Non-GAAP Financial Measures, and other provisions of the Securities Exchange Act of 1934, as amended (the Exchange Act), define and prescribe the conditions for use of certain non-GAAP financial information. These Non-GAAP Financial Measures are used in addition to and in conjunction with results presented in accordance with GAAP. These Non-GAAP Financial Measures should not be relied upon to the exclusion of GAAP financial measures. These Non-GAAP Financial Measures reflect an additional way of viewing aspects of our operations that, when viewed with our GAAP results and the accompanying reconciliations to corresponding GAAP financial measures, provide a more complete understanding of factors and trends affecting our business.
We believe the presentation of certain Non-GAAP Financial Measures are useful to investors and other external users of our financial statements regarding our results of operations because:
•they are widely used by investors and analysts in our industry as a supplemental measure to evaluate the overall performance of companies in our industry without regard to items such as other expense, net and depreciation and amortization, which can vary substantially from company to company depending on the book value of assets, capital structure and the method by which assets were acquired; and
•they help investors evaluate and compare the results of our operations from period to period by removing the impact of our capital structure and asset base from our operating results.
We use the Non-GAAP Financial Measures:
•as measurements of our operating performance to assist us in comparing our operating performance on a consistent basis;
•to allocate resources to enhance the financial performance of our business;
•to assess the value of a potential acquisition;
•to assess the value of a transformed operation's performance;
•to evaluate the effectiveness of our operational strategies; and
•to compare our operating performance to that of our competitors.
We use certain Non-GAAP Financial Measures to compare the operating performance of each operation. These measures are useful in this regard because they do not include such costs as other expense, income taxes, depreciation and amortization expense, which may vary from period-to-period depending upon various factors, including the method used to finance operations, the amount of debt that we have incurred, whether an operation is owned or leased, the date of acquisition of a facility or business, and the tax law of the state in which a business unit operates.
We also establish compensation programs and bonuses for our leaders that are partially based upon the achievement of Adjusted EBITDAR targets.
Despite the importance of these measures in analyzing our underlying business, designing incentive compensation and for our goal setting, the Non-GAAP Financial Measures have no standardized meaning defined by GAAP. Therefore, certain of our Non-GAAP Financial Measures have limitations as analytical tools, and they should not be considered in isolation, or as a substitute for analysis of our results as reported in accordance with GAAP. Some of these limitations are:
•they do not reflect our current or future cash requirements for capital expenditures or contractual commitments;
•they do not reflect changes in, or cash requirements for, our working capital needs;
•they do not reflect the interest expense, or the cash requirements necessary to service interest or principal payments, on our debt;
•they do not reflect rent expenses, which are necessary to operate our leased operations, in the case of Adjusted EBITDAR;
•they do not reflect any income tax payments we may be required to make;
•although depreciation and amortization are non-cash charges, the assets being depreciated and amortized will often have to be replaced in the future, and do not reflect any cash requirements for such replacements; and
•other companies in our industry may calculate these measures differently than we do, which may limit their usefulness as comparative measures.
77
We compensate for these limitations by using them only to supplement net income on a basis prepared in accordance with GAAP in order to provide a more complete understanding of the factors and trends affecting our business.
Management strongly encourages investors to review our consolidated financial statements in their entirety and to not rely on any single financial measure. Because these Non-GAAP Financial Measures are not standardized, it may not be possible to compare these financial measures with other companies’ Non-GAAP financial measures having the same or similar names. These Non-GAAP Financial Measures should not be considered a substitute for, nor superior to, financial results and measures determined or calculated in accordance with GAAP. We strongly urge you to review the reconciliation of income from operations to the Non-GAAP Financial Measures in the table below, along with our unaudited consolidated financial statements and related notes included elsewhere in this document.
We use the following Non-GAAP financial measures that we believe are useful to investors as key valuation and operating performance measures:
PERFORMANCE MEASURES
EBITDA
We believe EBITDA is useful to investors in evaluating our operating performance because it helps investors evaluate and compare the results of our operations from period to period by removing the impact of our asset base (depreciation and amortization expense) from our operating results.
We calculate EBITDA as net income, adjusted for net losses attributable to noncontrolling interest, before (a) other expense, net, (b) provision for income taxes, and (c) depreciation and amortization.
Adjusted EBITDA
We adjust EBITDA when evaluating our performance because we believe that the exclusion of certain additional items described below provides useful supplemental information to investors regarding our ongoing operating performance, in the case of Adjusted EBITDA. We believe that the presentation of Adjusted EBITDA, when combined with EBITDA and GAAP net income attributable to The Ensign Group, Inc., is beneficial to an investor’s complete understanding of our operating performance.
Adjusted EBITDA is EBITDA adjusted for non-core business items, which for the reported periods includes, to the extent applicable:
•stock-based compensation expense;
•real estate transactions and other related costs;
•legal finding;
•acquisition related costs;
•costs incurred related to new systems implementation;
•results related to operations not at full capacity; and
•gain on sale of assets and business interruptions recoveries.
Funds from Operations (FFO)
We consider FFO to be a useful supplemental measure of the operating performance of Standard Bearer. Historical cost accounting for real estate assets in accordance with U.S. GAAP implicitly assumes that the value of real estate assets diminishes predictably over time as evidenced by the provision for depreciation. However, since real estate values have historically risen or fallen with market conditions, many real estate investors and analysts have considered presentations of operating results for real estate companies that use historical cost accounting to be insufficient. In response, the National Association of Real Estate Investment Trusts (NAREIT) created FFO as a supplemental measure of operating performance for REITs, which excludes historical cost depreciation from net income. We define (in accordance with the definition used by NAREIT) FFO to consist of Standard Bearer segment income, excluding depreciation and amortization related to real estate, gains or losses from the sale of real estate, insurance recoveries related to real estate and impairment of depreciable real estate assets.
78
VALUATION MEASURE
Adjusted EBITDAR
We use Adjusted EBITDAR as one measure in determining the value of prospective acquisitions. It is also a commonly used measure by our management, research analysts and investors, to compare the enterprise value of different companies in the healthcare industry, without regard to differences in capital structures and leasing arrangements. Adjusted EBITDAR is a financial valuation measure that is not specified in GAAP. This measure is not displayed as a performance measure as it excludes rent expense, which is a normal and recurring operating expense, and is therefore presented only for the current period.
The adjustments made and previously described in the computation of Adjusted EBITDA are also made when computing Adjusted EBITDAR. We calculate Adjusted EBITDAR by excluding rent-cost of services from Adjusted EBITDA.
We believe the use of Adjusted EBITDAR allows the investor to compare operational results of companies who have operating and capital leases. A significant portion of capital lease expenditures are recorded in interest, whereas operating lease expenditures are recorded in rent expense.
The table below reconciles net income to EBITDA, Adjusted EBITDA and Adjusted EBITDAR for the periods presented:
| Year Ended December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
Consolidated statements of income data: | (In thousands) | ||||||||||
| Net income | $ | 224,652 | $ | 197,725 | |||||||
Less: net (loss) income attributable to noncontrolling interests | (29) | 3,073 | |||||||||
| Add: Other expense, net | 7,736 | 2,461 | |||||||||
Provision for income taxes | 64,437 | 60,279 | |||||||||
| Depreciation and amortization | 62,355 | 55,985 | |||||||||
| EBITDA | $ | 359,209 | $ | 313,377 | |||||||
| Stock-based compensation | 22,720 | 18,678 | |||||||||
Real estate transactions and other related costs(a) | — | 5,689 | |||||||||
Legal finding(b) | 4,280 | — | |||||||||
Gain on sale of assets and business interruptions recoveries | (4,380) | (2,365) | |||||||||
| Results related to operations not at full capacity | — | 585 | |||||||||
Acquisition related costs(c) | 669 | 384 | |||||||||
Costs incurred related to new systems implementation | 1,072 | 186 | |||||||||
| Rent related to items above | — | 38 | |||||||||
| Adjusted EBITDA | $ | 383,570 | $ | 336,572 | |||||||
| Rent—cost of services | 153,049 | 139,371 | |||||||||
| Less: rent related to items above | — | (38) | |||||||||
| Adjusted rent | 153,049 | 139,333 | |||||||||
| Adjusted EBITDAR | $ | 536,619 | |||||||||
(a) Real estate transactions and other related costs include costs incurred related to the formation of Standard Bearer and other real estate related activities.
(b) Legal finding against our non-emergent transportation subsidiary.
(c) Costs incurred to acquire operations that are not capitalizable.
79
Year Ended December 31, 2022 Compared to the Year Ended December 31, 2021
The following table sets forth details of operating results for our revenue and earnings, and their respective components, by our reportable segment for the periods indicated:
| Year Ended December 31, 2022 | ||||||||||||||||||||||||||||||||
| Skilled Services | Standard Bearer | All Other | Eliminations | Consolidated | ||||||||||||||||||||||||||||
| Total revenue | $ | 2,906,215 | $ | 72,937 | $ | 122,610 | $ | (76,294) | $ | 3,025,468 | ||||||||||||||||||||||
| Total expenses, including other expense, net | 2,497,483 | 45,066 | 273,391 | (76,294) | 2,739,646 | |||||||||||||||||||||||||||
| Segment income (loss) | 408,732 | 27,871 | (150,781) | — | 285,822 | |||||||||||||||||||||||||||
| Gain from sale of real estate | 3,267 | |||||||||||||||||||||||||||||||
| Income before provision for income taxes | $ | 289,089 | ||||||||||||||||||||||||||||||
| Year Ended December 31, 2021 | ||||||||||||||||||||||||||||||||
| Skilled Services | Standard Bearer | All Other | Eliminations | Consolidated | ||||||||||||||||||||||||||||
| Total revenue | $ | 2,523,234 | $ | 58,127 | $ | 102,685 | $ | (56,585) | $ | 2,627,461 | ||||||||||||||||||||||
| Total expenses, including other expense, net | 2,149,631 | 26,251 | 250,600 | (56,585) | 2,369,897 | |||||||||||||||||||||||||||
| Segment income (loss) | 373,603 | 31,876 | (147,915) | — | 257,564 | |||||||||||||||||||||||||||
Gain from sale of real estate | 440 | |||||||||||||||||||||||||||||||
| Income before provision for income taxes | $ | 258,004 | ||||||||||||||||||||||||||||||
Our total revenue increased $398.0 million, or 15.1%, compared to the year ended December 31, 2021. The increase in revenue was primarily driven by an increase in occupancy from our skilled services operations along with the impact of acquisitions. Total revenue from operations acquired on or subsequent to January 1, 2022 increased our consolidated revenue by $123.9 million during the year ended December 31, 2022, when compared to the same period in 2021. In addition, we recorded $81.8 million of state relief revenue during the year ended in 2022 compared to $75.2 million in 2021, which directly correlated to the additional COVID-19 related expenses incurred. All state relief revenue is included in Medicaid revenue.
Skilled Services Segment
Revenue
The following table presents the skilled services revenue and key performance metrics by category during the years ended December 31, 2022 and 2021:
| Year Ended December 31, | |||||||||||||||||||||||
| 2022 | 2021 | Change | % Change | ||||||||||||||||||||
| TOTAL FACILITY RESULTS: | (Dollars in thousands) | ||||||||||||||||||||||
| Skilled services revenue | $ | 2,906,215 | 2,523,234 | $ | 382,981 | 15.2 | % | ||||||||||||||||
| Number of facilities at period end | 234 | 211 | 23 | 10.9 | % | ||||||||||||||||||
| Number of campuses at period end* | 26 | 25 | 1 | 4.0 | % | ||||||||||||||||||
| Actual patient days | 7,243,781 | 6,478,810 | 764,971 | 11.8 | % | ||||||||||||||||||
| Occupancy percentage — Operational beds | 75.3 | % | 72.8 | % | 2.5 | % | |||||||||||||||||
| Skilled mix by nursing days | 31.8 | % | 31.7 | % | 0.1 | % | |||||||||||||||||
| Skilled mix by nursing revenue | 52.0 | % | 52.3 | % | (0.3) | % | |||||||||||||||||
80
| Year Ended December 31, | |||||||||||||||||||||||
| 2022 | 2021 | Change | % Change | ||||||||||||||||||||
SAME FACILITY RESULTS:(1) | (Dollars in thousands) | ||||||||||||||||||||||
| Skilled services revenue | $ | 2,237,100 | $ | 2,084,537 | $ | 152,563 | 7.3 | % | |||||||||||||||
| Number of facilities at period end | 167 | 167 | — | — | % | ||||||||||||||||||
| Number of campuses at period end* | 20 | 20 | — | — | % | ||||||||||||||||||
| Actual patient days | 5,450,136 | 5,269,464 | 180,672 | 3.4 | % | ||||||||||||||||||
| Occupancy percentage — Operational beds | 76.4 | % | 73.9 | % | 2.5 | % | |||||||||||||||||
| Skilled mix by nursing days | 33.7 | % | 33.1 | % | 0.6 | % | |||||||||||||||||
| Skilled mix by nursing revenue | 53.9 | % | 53.8 | % | 0.1 | % | |||||||||||||||||
| Year Ended December 31, | |||||||||||||||||||||||
| 2022 | 2021 | Change | % Change | ||||||||||||||||||||
TRANSITIONING FACILITY RESULTS:(2) | (Dollars in thousands) | ||||||||||||||||||||||
| Skilled services revenue | $ | 381,003 | $ | 336,338 | $ | 44,665 | 13.3 | % | |||||||||||||||
| Number of facilities at period end | 27 | 27 | — | — | % | ||||||||||||||||||
| Number of campuses at period end* | 5 | 5 | — | — | % | ||||||||||||||||||
| Actual patient days | 1,002,904 | 929,058 | 73,846 | 7.9 | % | ||||||||||||||||||
| Occupancy percentage — Operational beds | 74.9 | % | 69.4 | % | 5.5 | % | |||||||||||||||||
| Skilled mix by nursing days | 27.5 | % | 26.1 | % | 1.4 | % | |||||||||||||||||
| Skilled mix by nursing revenue | 47.4 | % | 46.3 | % | 1.1 | % | |||||||||||||||||
| Year Ended December 31, | |||||||||||||||||||||||
| 2022 | 2021 | Change | % Change | ||||||||||||||||||||
RECENTLY ACQUIRED FACILITY RESULTS:(3) | (Dollars in thousands) | ||||||||||||||||||||||
| Skilled services revenue | $ | 288,112 | $ | 102,359 | $ | 185,753 | NM | ||||||||||||||||
| Number of facilities at period end | 40 | 17 | 23 | NM | |||||||||||||||||||
| Number of campuses at period end* | 1 | — | 1 | NM | |||||||||||||||||||
| Actual patient days | 790,741 | 280,288 | 510,453 | NM | |||||||||||||||||||
| Occupancy percentage — Operational beds | 69.4 | % | 66.2 | % | NM | ||||||||||||||||||
| Skilled mix by nursing days | 23.5 | % | 22.4 | % | NM | ||||||||||||||||||
| Skilled mix by nursing revenue | 42.3 | % | 42.3 | % | NM | ||||||||||||||||||
*Campus represents a facility that offers both skilled nursing and senior living services. Revenue and expenses related to skilled nursing and senior living services have been allocated and recorded in the respective operating segment. In 2022, we converted three skilled nursing facilities into campuses.
(1)Same Facility results represent all facilities purchased prior to January 1, 2019.
(2)Transitioning Facility results represent all facilities purchased from January 1, 2019 to December 31, 2020.
(3)Recently Acquired Facility (Acquisitions) results represent all facilities purchased on or subsequent to January 1, 2021.
Skilled services revenue increased $383.0 million, or 15.2%, compared to the year ended December 31, 2021. Of the $383.0 million increase, the primary changes were from increases in Medicaid custodial revenue of $151.2 million, or 15.0%, Medicare revenue of $105.1 million, or 14.4%, managed care revenue of $69.0 million, or 15.1%, private revenue of $29.6 million, or 18.5% and Medicaid skilled revenue of $28.1 million, or 16.3%.
The increase in skilled services revenue was primarily driven by strong performance across our existing skilled services operations as our census continued to recover in fiscal year 2022 and the impact of operation expansions in 2022. Our consolidated occupancy increased by 2.5% and our skilled nursing days increased by 0.1% compared to 2021.
81
Revenue in our Same Facilities increased $152.6 million, or 7.3%, compared to 2021, due to increases in occupancy and skilled mix. Our diligent efforts to strengthen our partnership with various managed care organizations, hospitals and the local communities we operate in, increased our occupancy by 2.5% to 76.4%. Managed care and Medicare skilled days increased by 6.4% and 5.5%, respectively, coupled with an increase in our skilled revenue daily rate of 2.3%, resulting in an increase in skilled mix revenue.
Revenue generated by our Transitioning Facilities increased $44.7 million, or 13.3%, primarily due to improved occupancy growth of 5.5% and an increase in skilled mix days of 1.4%, compared to 2021, demonstrating our ability to transition these healthcare operations toward higher acuity patients. Skilled mix revenue increased by 1.1%, mainly from the increases in managed care and Medicare days of 22.3% and 8.6%, respectively, coupled with an increase in our skilled revenue daily rate of 1.7%.
Skilled services revenue generated by facilities purchased on or subsequent to January 1, 2021 (Recently Acquired Facilities) increased by approximately $185.8 million compared to the year ended December 31, 2021. The increases are primarily due to the expansion of 24 operations between January 1, 2022 and December 31, 2022 across six states.
In the future, if we acquire additional facilities that are underperforming and need to be turned around or invest in start-up operations, we expect to see lower occupancy rates and skilled mix and these metrics are expected to vary from period to period based upon the maturity of the facilities within our portfolio. Historically, we have generally experienced lower occupancy rates and lower skilled mix at Recently Acquired Facilities and therefore, we anticipate generally lower overall occupancy during years of growth.
The following table reflects the change in skilled nursing average daily revenue rates by payor source, excluding services that are not covered by the daily rate (1):
| Year Ended December 31, | |||||||||||||||||||||||||||||||||||||||||||||||
| Same Facility | Transitioning | Acquisitions | Total | ||||||||||||||||||||||||||||||||||||||||||||
| 2022 | 2021 | 2022 | 2021 | 2022 | 2021 | 2022 | 2021 | ||||||||||||||||||||||||||||||||||||||||
| SKILLED NURSING AVERAGE DAILY REVENUE RATES | |||||||||||||||||||||||||||||||||||||||||||||||
| Medicare | $ | 693.31 | $ | 687.26 | $ | 690.20 | $ | 681.34 | $ | 675.96 | $ | 707.03 | $ | 691.25 | $ | 687.18 | |||||||||||||||||||||||||||||||
| Managed care | 513.80 | 503.36 | 476.71 | 463.89 | 502.48 | 510.88 | 508.53 | 498.97 | |||||||||||||||||||||||||||||||||||||||
| Other skilled | 582.84 | 543.06 | 461.46 | 411.41 | 477.86 | 558.26 | 563.56 | 534.40 | |||||||||||||||||||||||||||||||||||||||
| Total skilled revenue | 599.02 | 585.58 | 578.03 | 568.30 | 583.74 | 624.26 | 595.26 | 584.72 | |||||||||||||||||||||||||||||||||||||||
| Medicaid | 262.11 | 251.35 | 245.74 | 234.38 | 245.87 | 245.52 | 257.67 | 248.41 | |||||||||||||||||||||||||||||||||||||||
| Private and other payors | 254.06 | 238.33 | 230.40 | 227.98 | 235.50 | 251.92 | 248.54 | 237.21 | |||||||||||||||||||||||||||||||||||||||
Total skilled nursing revenue | $ | 374.97 | $ | 360.80 | $ | 335.41 | $ | 320.95 | $ | 324.40 | $ | 330.88 | $ | 363.97 | $ | 353.79 | |||||||||||||||||||||||||||||||
(1) These rates exclude additional FMAP and other state relief funding and include sequestration reversal of 1% for the second quarter in 2022 and 2% for the first quarter of 2022 and the year ended December 31, 2021.
Our Medicare daily rates at Same Facilities and Transitioning Facilities increased by 0.9% and 1.3%, respectively, compared to the year ended December 31, 2021. The increase is attributable to the 2.7% net market basket increase that became effective in October 2022 offset by the removal of sequestration suspension. In 2022, Medicare daily rates includes three months of sequestration suspension of 1%, three months of sequestration suspension of 2% and six months of no sequestration suspension compared to the sequestration suspension of 2% that was in place for the entire year of 2021.
Our average Medicaid rates increased 3.7% due to state reimbursement increases and our participation in supplemental Medicaid payment programs and quality improvement programs in various states. Medicaid rates exclude the amount of state relief revenue we recorded.
Payor Sources as a Percentage of Skilled Nursing Services — We use our skilled mix as a measure of the quality of reimbursements we receive at our affiliated skilled nursing facilities over various periods.
82
The following tables set forth our percentage of skilled nursing patient revenue and days by payor source:
| Year Ended December 31, | |||||||||||||||||||||||||||||||||||||||||||||||
| Same Facility | Transitioning | Acquisitions | Total | ||||||||||||||||||||||||||||||||||||||||||||
| 2022 | 2021 | 2022 | 2021 | 2022 | 2021 | 2022 | 2021 | ||||||||||||||||||||||||||||||||||||||||
| PERCENTAGE OF SKILLED NURSING REVENUE | |||||||||||||||||||||||||||||||||||||||||||||||
| Medicare | 25.6 | % | 25.9 | % | 27.2 | % | 27.9 | % | 24.4 | % | 25.2 | % | 25.7 | % | 26.1 | % | |||||||||||||||||||||||||||||||
| Managed care | 19.6 | 19.4 | 16.8 | 15.1 | 10.6 | 9.0 | 18.3 | 18.4 | |||||||||||||||||||||||||||||||||||||||
| Other skilled | 8.7 | 8.5 | 3.4 | 3.3 | 7.3 | 8.1 | 8.0 | 7.8 | |||||||||||||||||||||||||||||||||||||||
| Skilled mix | 53.9 | 53.8 | 47.4 | 46.3 | 42.3 | 42.3 | 52.0 | 52.3 | |||||||||||||||||||||||||||||||||||||||
| Private and other payors | 7.0 | 6.8 | 8.0 | 7.7 | 6.9 | 6.1 | 7.0 | 6.9 | |||||||||||||||||||||||||||||||||||||||
| Medicaid | 39.1 | 39.4 | 44.6 | 46.0 | 50.8 | 51.6 | 41.0 | 40.8 | |||||||||||||||||||||||||||||||||||||||
| TOTAL SKILLED NURSING | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | |||||||||||||||||||||||||||||||
| Year Ended December 31, | |||||||||||||||||||||||||||||||||||||||||||||||
| Same Facility | Transitioning | Acquisitions | Total | ||||||||||||||||||||||||||||||||||||||||||||
| 2022 | 2021 | 2022 | 2021 | 2022 | 2021 | 2022 | 2021 | ||||||||||||||||||||||||||||||||||||||||
| PERCENTAGE OF SKILLED NURSING DAYS | |||||||||||||||||||||||||||||||||||||||||||||||
| Medicare | 13.9 | % | 13.6 | % | 13.2 | % | 13.2 | % | 11.7 | % | 11.8 | % | 13.5 | % | 13.5 | % | |||||||||||||||||||||||||||||||
| Managed care | 14.3 | 13.9 | 11.8 | 10.4 | 6.9 | 5.8 | 13.1 | 13.0 | |||||||||||||||||||||||||||||||||||||||
| Other skilled | 5.5 | 5.6 | 2.5 | 2.5 | 4.9 | 4.8 | 5.2 | 5.2 | |||||||||||||||||||||||||||||||||||||||
| Skilled mix | 33.7 | 33.1 | 27.5 | 26.1 | 23.5 | 22.4 | 31.8 | 31.7 | |||||||||||||||||||||||||||||||||||||||
| Private and other payors | 10.3 | 10.3 | 11.6 | 11.0 | 9.5 | 8.1 | 10.3 | 10.2 | |||||||||||||||||||||||||||||||||||||||
| Medicaid | 56.0 | 56.6 | 60.9 | 62.9 | 67.0 | 69.5 | 57.9 | 58.1 | |||||||||||||||||||||||||||||||||||||||
| TOTAL SKILLED NURSING | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | 100.0 | % | |||||||||||||||||||||||||||||||
Cost of Services
The following table sets forth total cost of services for our skilled services segment for the periods indicated (dollars in thousands):
| Year Ended December 31, | Change | |||||||||||||||||||||||||
| 2022 | 2021 | $ | % | |||||||||||||||||||||||
| Cost of service | $ | 2,267,691 | $ | 1,944,461 | $ | 323,230 | 16.6 | % | ||||||||||||||||||
| Revenue percentage | 78.0 | % | 77.1 | % | 0.9 | % | ||||||||||||||||||||
Cost of services related to our skilled services segment increased by $323.2 million, or 16.6%, due to additional costs at new operation expansions, which accounted for $147.7 million of the increase to cost of services. The remaining increases are mainly due to higher staffing expenses. As the result of COVID-19 variants, our operations experienced staffing constraints due to isolation requirements and COVID-19 exposure, which resulted in additional overtime, benefits and bonuses to our staff as well as higher use of contracted labor. The increase in labor costs is offset by cost management in non-clinical expenses. Cost of services as a percentage of revenue increased to 78.0% from 77.1%.
83
Standard Bearer
| Year Ended December 31, | Change | |||||||||||||||||||||||||
| 2022 | 2021 | $ | % | |||||||||||||||||||||||
| (Dollars in thousands) | ||||||||||||||||||||||||||
| Rental revenue generated from third-party tenants | $ | 14,970 | 13,962 | $ | 1,008 | 7.2 | % | |||||||||||||||||||
| Rental revenue generated from Ensign affiliated operations | 57,967 | 44,165 | 13,802 | 31.3 | ||||||||||||||||||||||
| TOTAL RENTAL REVENUE | $ | 72,937 | $ | 58,127 | $ | 14,810 | 25.5 | % | ||||||||||||||||||
| Segment income | 27,871 | 31,876 | (4,005) | (12.6) | ||||||||||||||||||||||
| Depreciation and amortization | 21,613 | 17,558 | 4,055 | 23.1 | ||||||||||||||||||||||
| FFO | $ | 49,484 | $ | 49,434 | $ | 50 | 0.1 | % | ||||||||||||||||||
Rental revenue — Standard Bearer's rental revenue, including revenue generated from our affiliated facilities, increased by $14.8 million, or 25.5% to $72.9 million, compared to the year ended December 31, 2021. The increase in revenue is primarily attributable to ten real estate purchases as well as annual rent increases since the year ended December 31, 2021.
Segment income — Standard Bearer's segment income decreased by 12.6% to $27.9 million, compared to the year ended December 31, 2021. The decrease is primarily attributable to increases in interest expense as a result of intercompany debt arrangements used to fund real estate acquisitions, management fee expense associated with the intercompany agreements between Standard Bearer and the Service Center and depreciation and amortization offset by increases in rental revenue as a result of the real estate acquisitions.
FFO — Standard Bearer's FFO increased by 0.1% to $49.5 million, compared to the year ended December 31, 2021. The increase is similar to the change in segment income with the exclusion of depreciation and amortization. Excluding the expenses entered into in 2022, FFO increased by 26.4%.
All Other Revenue
Our other revenue increased by $19.9 million, or 19.4% to $122.6 million, compared to the year ended December 31, 2021. Other revenue for 2022 includes senior living revenue of $67.4 million and revenue from other ancillary services of $47.8 million and rental income of $7.4 million. The increase in other revenue is attributable to our senior living operation expansions in 2022.
Consolidated Financial Expenses
Rent — cost of services — Our rent — cost of services as a percentage of total revenue decreased by 0.2% to 5.1%, primarily due to the growth in revenue outpacing the increase in rent expense and as our operation expansions include the acquisition of the related real estate properties.
General and administrative expense — General and administrative expense increased $7.0 million or 4.6%, to $158.8 million. This increase was primarily due to increases in wages and benefits due to enhanced performance and growth. General and administrative expense as a percentage of revenue decreased by 0.6% to 5.2%, which demonstrates our refocused efforts on non-clinical spend management.
Depreciation and amortization — Depreciation and amortization expense increased $6.4 million, or 11.4%, to $62.4 million. This increase was primarily related to the additional depreciation and amortization incurred as a result of our newly acquired operations. Depreciation and amortization remained consistent at 2.1%, as a percentage of revenue.
Other expense, net — Other expense, net as a percentage of revenue increased by 0.2%, to 0.3%. Other expense primarily includes interest expense related to our debt and gain or loss on the deferred compensation investments. During the year ended December 31, 2022, we recorded a loss on those investments of $4.2 million compared to a gain of $1.6 million during the year ended December 31, 2021. There is an offsetting income and offsetting expense split between cost of services and general and administrative expenses in 2022 and 2021, respectively.
84
Provision for income taxes — Our effective tax rate was 22.3% for the year ended December 31, 2022, compared to 23.4% for the same period in 2021. The effective tax rate for both periods is driven by the impact of excess tax benefits from stock-based compensation, partially offset by non-deductible expenses. See Note 15, Income Taxes, in the Notes to the Consolidated Financial Statements for further discussion.
Liquidity and Capital Resources
Our primary sources of liquidity have historically been derived from our cash flows from operations and long-term debt secured by our real property and our Revolving Credit Facility. Our liquidity as of December 31, 2022 is impacted by cash generated from strong operational performance and increased acquisition and share repurchase activities.
Historically, we have primarily financed the majority of our acquisitions through mortgages on our properties, our Revolving Credit Facility and cash generated from operations. Cash paid to fund acquisitions was $101.1 million and $104.1 million for the years ended December 2022 and 2021, respectively. Total capital expenditures for property and equipment were $87.5 million and $69.6 million for the years ended December 31, 2022 and 2021, respectively. We currently have approximately $80.0 million budgeted for renovation projects for 2023. We believe our current cash balances, our cash flow from operations and the amounts available for borrowing under our Revolving Credit Facility will be sufficient to cover our operating needs for at least the next 12 months.
We may, in the future, seek to raise additional capital to fund growth, capital renovations, operations and other business activities, but such additional capital may not be available on acceptable terms, on a timely basis, or at all.
Our cash and cash equivalents as of December 31, 2022 consisted of bank term deposits, money market funds and U.S. Treasury bill related investments. In addition, as of December 31, 2022, we held investments of approximately $83.1 million. We believe our investments that were in an unrealized loss position as of December 31, 2022 do not require an allowance for expected credit losses, nor has any event occurred subsequent to that date that would indicate so.
As mentioned above, our primary sources of cash is from our ongoing operations. Our positive cash flows have supported our business and have allowed us to pay regular dividends to our stockholders. We currently anticipate that existing cash and total investments as of December 31, 2022, along with projected operating cash flows and available financing, will support our normal business operations for the foreseeable future.
On July 28, 2022, the Board of Directors approved a stock repurchase program pursuant to which we may repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from August 2, 2022. Under this program, we are authorized to repurchase our issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. The Company did not purchase any shares pursuant to this stock repurchase program in the year ended December 31, 2022. The share repurchase program does not obligate us to acquire any specific number of shares.
On February 9, 2022, the Board of Directors approved a stock repurchase program pursuant to which we could repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from February 10, 2022. Under this program, we were authorized to repurchase our issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. During the second quarter of 2022, we repurchased approximately 0.3 million shares of our common stock for $20.0 million. This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
On October 21, 2021, the Board of Directors approved a stock repurchase program pursuant to which we could repurchase up to $20.0 million of our common stock under the program for a period of approximately 12 months from October 29, 2021. Under this program, we were authorized to repurchase our issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. During the first quarter of 2022, we repurchased approximately 0.1 million shares of our common stock for $9.9 million. During the fourth quarter of 2021, we repurchased 0.1 million shares of our common stock for $10.1 million. This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
85
The following table presents selected data from our consolidated statement of cash flows for the periods presented:
| Year Ended December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| NET CASH PROVIDED BY/(USED IN): | (In thousands) | ||||||||||
| Operating activities | $ | 272,513 | $ | 275,684 | |||||||
| Investing activities | (186,182) | (173,907) | |||||||||
| Financing activities | (32,262) | (76,138) | |||||||||
| Net increase in cash and cash equivalents | 54,069 | 25,639 | |||||||||
| Cash and cash equivalents beginning of period | 262,201 | 236,562 | |||||||||
| Cash and cash equivalents at end of period | $ | 316,270 | $ | 262,201 | |||||||
Operating Activities
Cash provided by operating activities is net income adjusted for certain non-cash items and changes in operating assets and liabilities.
The $3.2 million decrease in cash provided by operating activities for the year ended December 31, 2022 compared to the same period in 2021 was primarily due to changes in working capital offset by higher net income. Changes in working capital were driven by timing of collections of accounts receivable and accrued wages and related liabilities.
Investing Activities
Investing cash flows consist primarily of capital expenditures, investment activities, insurance proceeds and cash used for acquisitions.
The $12.3 million increase in cash used in investing activities for the year ended December 31, 2022 compared to the same period in 2021, was primarily due to an increase in cash used for expansions and capital expenditures of $15.0 million partially offset by sale of assets.
Financing Activities
Financing cash flows consist primarily of payment of dividends to stockholders, issuance and repayment of short-term and long-term debt, payment for share repurchases, repayment of the Medicare Accelerated and Advance Payment Program funds and sale of subsidiary shares.
The $43.9 million decrease in cash used in financing activities for the year ended December 31, 2022 compared to the same period in 2021, was primarily due to $102.0 million of net repayments of the Medicare Accelerated and Advance Payment Program funds in 2021 and $6.7 million receipt of proceeds from the sale of preferred shares and common stock of Standard Bearer in 2022. This is offset by $19.8 million of share repurchases as part of our stock repurchase program in 2022 and $45.2 million in proceeds from HUD borrowings in the same period in 2021, that did not recur in 2022.
A discussion of our cash flows for the year ended December 31, 2020 is included in Part II, Item 7, Management’s Discussion and Analysis of Financial Condition and Results of Operations - Liquidity and Capital Resources, included in our Annual Report on Form 10-K for the year ended December 31, 2021 filed with the Securities and Exchange Commission on February 9, 2022.
86
Material cash requirements from known contractual and other obligations
Total long-term debt obligations outstanding as of the end of each fiscal year were as follows:
| December 31, | |||||||||||||||||||||||||||||
| 2022 | 2021 | 2020 | 2019 | 2018 | |||||||||||||||||||||||||
| (In thousands) | |||||||||||||||||||||||||||||
| Credit facilities and term loans | $ | — | $ | — | $ | — | $ | 210,000 | $ | 123,125 | |||||||||||||||||||
| Mortgage loan and promissory notes | 156,271 | 159,967 | 117,806 | 120,350 | 122,955 | ||||||||||||||||||||||||
| TOTAL | $ | 156,271 | $ | 159,967 | $ | 117,806 | $ | 330,350 | $ | 246,080 | |||||||||||||||||||
Significant contractual obligations as of December 31, 2022 were as follows, including the future periods in which payments are expected:
| 2023 | 2024 | 2025 | 2026 | 2027 | Thereafter | Total | ||||||||||||||||||||||||||||||||||||||
| (In thousands) | ||||||||||||||||||||||||||||||||||||||||||||
| Operating lease obligations | $ | 157,963 | $ | 157,630 | $ | 157,455 | $ | 157,380 | $ | 156,860 | $ | 1,456,411 | $ | 2,243,699 | ||||||||||||||||||||||||||||||
| Long-term debt obligations | 3,883 | 3,950 | 4,086 | 4,227 | 3,897 | 136,228 | 156,271 | |||||||||||||||||||||||||||||||||||||
| Interest payments on long-term debt | 4,754 | 4,623 | 4,487 | 4,346 | 4,207 | 58,527 | 80,944 | |||||||||||||||||||||||||||||||||||||
| TOTAL | $ | 166,600 | $ | 166,203 | $ | 166,028 | $ | 165,953 | $ | 164,964 | $ | 1,651,166 | $ | 2,480,914 | ||||||||||||||||||||||||||||||
Not included in the table above are our actuarially determined self-insured general and professional malpractice liability, workers' compensation and medical (including prescription drugs) and dental healthcare obligations, which are broken out between current and long-term liabilities in our financial statements included in this Annual Report on Form 10-K.
Credit Facility with a Lending Consortium Arranged by Truist
On April 8, 2022, we entered into the Amended Credit Agreement, which increased the amount of the revolving line of credit thereunder to $600.0 million in aggregate principal amount. The maturity date of the Revolving Credit Facility is April 8, 2027. Borrowings are supported by a lending consortium arranged by Truist. The interest rates applicable to loans under the Revolving Credit Facility are, at our option, equal to either a base rate plus a margin ranging from 0.25% to 1.25% per annum or SOFR plus a margin range from 1.25% to 2.25% per annum, based on the Consolidated Total Net Debt to Consolidated EBITDA ratio (as defined in the Amended Credit Agreement). In addition, we will pay a commitment fee on the unused portion of the commitments that will range from 0.20% to 0.40% per annum, depending on the Consolidated Total Net Debt to Consolidated EBITDA ratio.
Mortgage Loans and Promissory Notes
As of December 31, 2022, 23 of our subsidiaries have mortgage loans insured with HUD for an aggregate amount of $153.5 million, which subjects these subsidiaries to HUD oversight and periodic inspections. The mortgage loans bear effective interest rates at a range of 3.1% to 4.2%, including fixed interest rates at a range of 2.4% to 3.3% per annum. Amounts borrowed under the mortgage loans may be prepaid, subject to prepayment fees of the principal balance on the date of prepayment. For the majority of the loans, the prepayment fee is 10% during the first three years and is reduced by 3% in the fourth year of the loan, and is reduced by 1% per year for years five through ten of the loan. There is no prepayment penalty after year ten. The term of the mortgage loans are 25 to 35 years.
In addition to the HUD mortgage loans above, we have two promissory notes. The notes bear fixed interest rates of 6.3% and 5.3% per annum and the term of the notes are 10 months and 12 years, respectively. The 12 year note, which was used for an acquisition, is secured by the real property comprising the facility and the rent, issues and profits thereof, as well as all personal property used in the operation of the facility.
87
Operating Leases
As of December 31, 2022, 192 of our facilities are under long-term lease arrangements, of which 96 of the operations are under nine triple-net Master Leases and one stand-alone lease with CareTrust REIT, Inc. (CareTrust). The Master Leases consist of multiple leases, each with its own pool of properties, that have varying maturities and diversity in property geography. Under each master lease, our individual subsidiaries that operate those properties are the tenants and CareTrust's individual subsidiaries that own the properties subject to the Master Leases are the landlords. The rent structure under the Master Leases includes a fixed component, subject to annual escalation equal to the lesser of the percentage change in the Consumer Price Index (but not less than zero) or 2.5%. At our option, we can extend the Master Leases for two or three five-year renewal terms beyond the initial term, on the same terms and conditions. If we elect to renew the term of a Master Lease, the renewal will be effective as to all, but not less than all, of the leased property then subject to the Master Lease. Additionally, four of the 97 facilities leased from CareTrust include an option to purchase that we can exercise starting on December 1, 2024.
We also lease certain affiliated facilities and our administrative offices under non-cancelable operating leases, most of which have initial lease terms ranging from five to 20 years and is subject to annual escalation equal to the percentage change in the Consumer Price Index with a stated cap percentage. In addition, we lease certain of our equipment under non-cancelable operating leases with initial terms ranging from three to five years. Most of these leases contain renewal options, certain of which involve rent increases.
Fifty-eight of our affiliated facilities, excluding the facilities that are operated under the Master Leases from CareTrust, are operated under ten separate master lease arrangements. Under these master leases, a breach at a single facility could subject one or more of the other affiliated facilities covered by the same master lease to the same default risk. Failure to comply with Medicare and Medicaid provider requirements is a default under several of our leases, master lease agreements and debt financing instruments. In addition, other potential defaults related to an individual facility may cause a default of an entire master lease portfolio and could trigger cross-default provisions in our outstanding debt arrangements and other leases. With an indivisible lease, it is difficult to restructure the composition of the portfolio or economic terms of the lease without the consent of the landlord.
U.S. Department of Justice Civil Investigative Demand
On May 31, 2018, we received a Civil Investigative Demand (CID) from the U.S. Department of Justice stating that it is investigating to determine whether we have violated the False Claims Act and/or the Anti-Kickback Statute with respect to the relationships between certain of our skilled nursing facilities and persons who served as medical directors, advisory board participants or other referral sources. The CID covered the period from October 3, 2013 through 2018, and was limited in scope to ten of our Southern California skilled nursing facilities. In October 2018, the Department of Justice made an additional request for information covering the period of January 1, 2011 through 2018, relating to the same topic. As a general matter, our operating entities maintain policies and procedures to promote compliance with the False Claims Act, the Anti-Kickback Statute, and other applicable regulatory requirements. We have fully cooperated with the U.S. Department of Justice and promptly responded to its requests for information; in April 2020, we were advised that the U.S. Department of Justice declined to intervene in any subsequent action based on or related to the subject matter of this investigation.
Inflation
We have historically derived a substantial portion of our revenue from the Medicare program. We also derive revenue from state Medicaid and similar reimbursement programs. Payments under these programs generally provide for reimbursement levels that are adjusted for inflation annually based upon the state’s fiscal year for the Medicaid programs and in each October for the Medicare program. These adjustments may not continue in the future, and even if received, such adjustments may not reflect the actual increase in our costs for providing healthcare services.
Labor, supply expenses and capital expenditures make up a substantial portion of our cost of services. Those expenses can be subject to increase in periods of rising inflation and when labor shortages occur in the marketplace. To date, we have generally been able to implement cost control measures or obtain increases in reimbursement sufficient to offset increases in these expenses. There can be no assurance that we will be able to anticipate fully or otherwise respond to any future inflationary pressures.
88
Item 7A. QUANTITATIVE AND QUALITATIVE DISCLOSURES ABOUT MARKET RISK
Interest Rate Risk — We are exposed to risks associated with market changes in interest rates through our borrowing arrangements and investments. In particular, our Revolving Credit Facility exposes us to variability in interest payments due to changes in SOFR interest rates. We manage our exposure to this market risk by monitoring available financing alternatives. Our mortgages and promissory notes require principal and interest payments through maturity pursuant to amortization schedules.
Our mortgages generally contain provisions that allow us to make repayments earlier than the stated maturity date. In some cases, we are not allowed to make early repayment prior to a cutoff date. Where prepayment is permitted, we are generally allowed to make prepayments only at a premium which is often designed to preserve a stated yield to the note holder. These prepayment rights may afford us opportunities to mitigate the risk of refinancing our debts at maturity at higher rates by refinancing prior to maturity.
On April 8, 2022, we entered into the Amended Credit Agreement, with a revolving line of credit of up to $600.0 million in aggregate principal amount. The Amended Credit Agreement amended the reference for borrowings under the Revolving Credit Facility rate from LIBOR to SOFR. We have no outstanding borrowings under our Amended Credit Facility as of December 31, 2022 and January 30, 2023.
We have outstanding indebtedness under mortgage loans insured with HUD and two promissory notes to third parties of $156.3 million, all of which are at fixed interest rates.
Our cash and cash equivalents as of December 31, 2022 consisted of bank term deposits, money market funds and U.S. Treasury bill related investments. In addition, as of December 31, 2022, we held investments of approximately $83.1 million. We believe our investments that were in an unrealized loss position as of December 31, 2022 do not require an allowance for expected credit losses, nor has any event occurred subsequent to that date that would indicate so. Our market risk exposure is interest income sensitivity, which is affected by changes in the general level of U.S. interest rates. The primary objective of our investment activities is to preserve principal, while at the same time maximizing the income we receive from our investments without significantly increasing risk. Due to the low risk profile of our investment portfolio, an immediate 10.0% change in interest rates would not have a material effect on the fair market value of our portfolio. Accordingly, we would not expect our operating results or cash flows to be affected to any significant degree by the effect of a sudden change in market interest rates on our securities portfolio.
The above only incorporates those exposures that exist as of December 31, 2022 and does not consider those exposures or positions which could arise after that date. If we diversify our investment portfolio into securities and other investment alternatives, we may face increased risk and exposures as a result of interest risk and the securities markets in general.
89
Item 8. FINANCIAL STATEMENTS AND SUPPLEMENTARY DATA
THE ENSIGN GROUP, INC.
INDEX TO CONSOLIDATED FINANCIAL STATEMENTS
AND FINANCIAL STATEMENT SCHEDULE
| Consolidated Financial Statements: | |||||
90
REPORT OF INDEPENDENT REGISTERED PUBLIC ACCOUNTING FIRM
To the Stockholders and the Board of Directors of
The Ensign Group, Inc.
San Juan Capistrano, California
Opinion on the Financial Statements
We have audited the accompanying consolidated balance sheets of The Ensign Group, Inc. and subsidiaries (the "Company") as of December 31, 2022 and 2021, the related consolidated statements of income, shareholders' equity, and cash flows, for each of the three years in the period ended December 31, 2022, and the related notes (collectively referred to as the "financial statements"). In our opinion, the financial statements present fairly, in all material respects, the financial position of the Company as of December 31, 2022 and 2021, and the results of its operations and its cash flows for each of the three years in the period ended December 31, 2022, in conformity with accounting principles generally accepted in the United States of America.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the Company's internal control over financial reporting as of December 31, 2022, based on criteria established in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission and our report dated February 2, 2023, expressed an unqualified opinion on the Company's internal control over financial reporting.
Basis for Opinion
These financial statements are the responsibility of the Company's management. Our responsibility is to express an opinion on the Company's financial statements based on our audits. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audits in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether the financial statements are free of material misstatement, whether due to error or fraud. Our audits included performing procedures to assess the risks of material misstatement of the financial statements, whether due to error or fraud, and performing procedures that respond to those risks. Such procedures included examining, on a test basis, evidence regarding the amounts and disclosures in the financial statements. Our audits also included evaluating the accounting principles used and significant estimates made by management, as well as evaluating the overall presentation of the financial statements. We believe that our audits provide a reasonable basis for our opinion.
Critical Audit Matter
The critical audit matter communicated below is a matter arising from the current-period audit of the financial statements that was communicated or required to be communicated to the audit committee and that (1) relates to accounts or disclosures that are material to the financial statements and (2) involved our especially challenging, subjective, or complex judgments. The communication of critical audit matters does not alter in any way our opinion on the financial statements, taken as a whole, and we are not, by communicating the critical audit matter below, providing a separate opinion on the critical audit matter or on the accounts or disclosures to which it relates.
Self-Insurance Liabilities (General and Professional Liability Claims) - Refer to Notes 2 and 19 to the financial statements
Critical Audit Matter Description
The Company's self-insurance liabilities for general and professional liability claims totaled $87.0 million at December 31, 2022. The Company develops information about the size of the ultimate claims based on historical experience, current industry information, and actuarial analysis.
The determination of reserves for general and professional liability claims is highly subjective. Given the significant judgments in estimating the general and professional liability claims, we have determined this to be a critical audit matter. This required a high degree of auditor judgment and an increased extent of effort when performing audit procedures to evaluate the reasonableness of management estimates of reserves for open claims as well as for claims that are incurred but not reported (IBNR).
How the Critical Audit Matter Was Addressed in the Audit
Our audit procedures relating to management’s judgment regarding the estimation of the reserve for general and professional liability claims included the following, among others:
•We tested the effectiveness of controls over the reserve for general and professional liabilities, including those related to both the determination of reserves for open claims and estimation of the IBNR claims.
•We obtained an understanding of the factors considered and assumptions made by management and its external actuarial specialists in developing the estimate of the general and professional liability reserves, including the sources of data relevant to these factors and assumptions. We tested underlying claims data, including testing the completeness and accuracy of open cases handled by legal firms.
•We involved our actuarial specialists to assist in our evaluation of the methodologies applied by management's specialist and to assess the accuracy of the Company's reserves. We also compared the reserves recorded to an independent range developed by our actuarial specialists.
•We performed a retrospective review in which we compared the current portion of the total liability at the end of the prior year to actual paid claim emergence in the current year.
/s/ DELOITTE & TOUCHE LLP
February 2, 2023
We have served as the Company's auditor since 1999.
91
THE ENSIGN GROUP, INC.
CONSOLIDATED BALANCE SHEETS
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| (In thousands, except par values) | |||||||||||
| ASSETS | |||||||||||
| Current assets: | |||||||||||
| Cash and cash equivalents | $ | $ | |||||||||
Accounts receivable—less allowance for doubtful accounts of $ | |||||||||||
| Investments—current | |||||||||||
| Prepaid income taxes | |||||||||||
| Prepaid expenses and other current assets | |||||||||||
| Total current assets | |||||||||||
| Property and equipment, net | |||||||||||
| Right-of-use assets | |||||||||||
| Insurance subsidiary deposits and investments | |||||||||||
| Deferred tax assets | |||||||||||
| Restricted and other assets | |||||||||||
| Intangible assets, net | |||||||||||
| Goodwill | |||||||||||
| Other indefinite-lived intangibles | |||||||||||
| TOTAL ASSETS | $ | $ | |||||||||
| LIABILITIES AND EQUITY | |||||||||||
| Current liabilities: | |||||||||||
| Accounts payable | $ | $ | |||||||||
Accrued wages and related liabilities (Note 3) | |||||||||||
| Lease liabilities—current | |||||||||||
| Accrued self-insurance liabilities—current | |||||||||||
| Other accrued liabilities | |||||||||||
| Current maturities of long-term debt | |||||||||||
| Total current liabilities | |||||||||||
| Long-term debt—less current maturities | |||||||||||
| Long-term lease liabilities—less current portion | |||||||||||
| Accrued self-insurance liabilities—less current portion | |||||||||||
| Other long-term liabilities | |||||||||||
| TOTAL LIABILITIES | $ | $ | |||||||||
Commitments and contingencies (Notes 16, 18 and 21) | |||||||||||
| EQUITY | |||||||||||
| Ensign Group, Inc. stockholders' equity: | |||||||||||
Common stock: $ | |||||||||||
| Additional paid-in capital | |||||||||||
| Retained earnings | |||||||||||
Common stock in treasury, at cost, | ( | ( | |||||||||
| Total Ensign Group, Inc. stockholders' equity | |||||||||||
| Non-controlling interest | |||||||||||
| Total equity | $ | $ | |||||||||
| TOTAL LIABILITIES AND EQUITY | $ | $ | |||||||||
See accompanying notes to consolidated financial statements.
92
THE ENSIGN GROUP, INC.
CONSOLIDATED STATEMENTS OF INCOME
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| (In thousands, except per share data) | |||||||||||||||||
| REVENUE | |||||||||||||||||
| Service revenue | $ | $ | $ | ||||||||||||||
| Rental revenue | |||||||||||||||||
| TOTAL REVENUE | $ | $ | $ | ||||||||||||||
| Expense: | |||||||||||||||||
| Cost of services | |||||||||||||||||
| Rent—cost of services | |||||||||||||||||
| General and administrative expense | |||||||||||||||||
| Depreciation and amortization | |||||||||||||||||
| TOTAL EXPENSES | $ | $ | $ | ||||||||||||||
| Income from operations | |||||||||||||||||
| Other (expense) income: | |||||||||||||||||
| Interest expense | ( | ( | ( | ||||||||||||||
| Other income | |||||||||||||||||
| Other expense, net | $ | ( | $ | ( | $ | ( | |||||||||||
| Income before provision for income taxes | |||||||||||||||||
| Provision for income taxes | |||||||||||||||||
| NET INCOME | $ | $ | $ | ||||||||||||||
| Less: | |||||||||||||||||
| Net (loss) income attributable to noncontrolling interests | ( | ||||||||||||||||
| Net income attributable to The Ensign Group, Inc. | $ | $ | $ | ||||||||||||||
| NET INCOME PER SHARE ATTRIBUTABLE TO THE ENSIGN GROUP INC. | |||||||||||||||||
| Basic | $ | $ | $ | ||||||||||||||
| Diluted | $ | $ | $ | ||||||||||||||
| WEIGHTED AVERAGE COMMON SHARES OUTSTANDING | |||||||||||||||||
| Basic | |||||||||||||||||
| Diluted | |||||||||||||||||
See accompanying notes to consolidated financial statements.
93
THE ENSIGN GROUP, INC.
CONSOLIDATED STATEMENTS OF STOCKHOLDERS' EQUITY
| Common Stock | Additional Paid-In Capital | Retained Earnings | Treasury Stock | Non-Controlling Interest | |||||||||||||||||||||||||||||||||||||||||||
| (In thousands) | Shares | Amount | Shares | Amount | Total | ||||||||||||||||||||||||||||||||||||||||||
| BALANCE - JANUARY 1, 2020 | $ | $ | $ | $ | ( | $ | $ | ||||||||||||||||||||||||||||||||||||||||
| Issuance of common stock to employees and directors resulting from the exercise of stock options and grant of stock awards | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||||
| Issuance of restricted stock, net of forfeitures | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||||
| Shares of common stock used to satisfy tax withholding obligations | ( | — | — | — | ( | — | ( | ||||||||||||||||||||||||||||||||||||||||
Dividends declared ($ | — | — | — | ( | — | — | — | ( | |||||||||||||||||||||||||||||||||||||||
| Employee stock award compensation | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
Repurchase of common stock (Note 22) | ( | — | — | — | ( | — | ( | ||||||||||||||||||||||||||||||||||||||||
| Net income attributable to noncontrolling interest | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| Distribution to noncontrolling interest holder | — | — | — | — | — | — | ( | ( | |||||||||||||||||||||||||||||||||||||||
| Net income attributable to the Ensign Group, Inc. | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| BALANCE - DECEMBER 31, 2020 | $ | $ | $ | $ | ( | $ | $ | ||||||||||||||||||||||||||||||||||||||||
| Issuance of common stock to employees and directors resulting from the exercise of stock options | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Issuance of restricted stock, net of forfeitures | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Shares of common stock used to satisfy tax withholding obligations | ( | — | — | — | ( | — | ( | ||||||||||||||||||||||||||||||||||||||||
Dividends declared ($ | — | — | — | ( | — | — | — | ( | |||||||||||||||||||||||||||||||||||||||
| Employee stock award compensation | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
Repurchase of common stock (Note 22) | ( | — | — | — | ( | — | ( | ||||||||||||||||||||||||||||||||||||||||
| Deconsolidation of an ancillary business | — | — | — | — | — | — | ( | ( | |||||||||||||||||||||||||||||||||||||||
| Capital contribution from noncontrolling interest holder | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| Net income attributable to noncontrolling interest | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| Distribution to noncontrolling interest holder | — | — | — | — | — | — | ( | ( | |||||||||||||||||||||||||||||||||||||||
| Net income attributable to the Ensign Group, Inc. | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| BALANCE - DECEMBER 31, 2021 | $ | $ | $ | $ | ( | $ | $ | ||||||||||||||||||||||||||||||||||||||||
| Issuance of common stock to employees and directors resulting from the exercise of stock options | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||||
| Issuance of restricted stock, net of forfeitures | — | — | — | — | — | ||||||||||||||||||||||||||||||||||||||||||
| Shares of common stock used to satisfy tax withholding obligations | ( | — | — | — | ( | — | ( | ||||||||||||||||||||||||||||||||||||||||
Dividends declared ($ | — | — | — | ( | — | — | — | ( | |||||||||||||||||||||||||||||||||||||||
| Employee stock award compensation | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
Repurchase of common stock (Note 22) | ( | — | — | — | ( | — | ( | ||||||||||||||||||||||||||||||||||||||||
| Acquisition of noncontrolling interest shares | — | — | ( | — | — | — | ( | ||||||||||||||||||||||||||||||||||||||||
| Issuance of noncontrolling interests through subsidiary equity plan | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| Net loss attributable to noncontrolling interest | — | — | — | — | — | — | ( | ( | |||||||||||||||||||||||||||||||||||||||
| Distribution to noncontrolling interest holder and other changes | — | — | — | — | — | ( | ( | ||||||||||||||||||||||||||||||||||||||||
| Net income attributable to the Ensign Group, Inc. | — | — | — | — | — | — | |||||||||||||||||||||||||||||||||||||||||
| BALANCE - DECEMBER 31, 2022 | $ | $ | $ | $ | ( | $ | $ | ||||||||||||||||||||||||||||||||||||||||
See accompanying notes to consolidated financial statements.
94
THE ENSIGN GROUP, INC.
CONSOLIDATED STATEMENTS OF CASH FLOWS
| Year Ended December 31, | |||||||||||||||||
| (In thousands) | 2022 | 2021 | 2020 | ||||||||||||||
| Cash flows from operating activities: | |||||||||||||||||
| Net income | $ | $ | $ | ||||||||||||||
| Adjustments to reconcile net income to net cash provided by operating activities: | |||||||||||||||||
| Depreciation and amortization | |||||||||||||||||
| Impairment of long-lived assets | |||||||||||||||||
| Amortization of deferred financing fees | |||||||||||||||||
| Non-cash leasing arrangement | |||||||||||||||||
| Write-off of deferred financing fees | |||||||||||||||||
| Deferred income taxes | ( | ( | ( | ||||||||||||||
| Provision for doubtful accounts | |||||||||||||||||
| Stock-based compensation | |||||||||||||||||
| Cash received from insurance proceeds | |||||||||||||||||
| Gain on sale of assets | ( | ( | |||||||||||||||
| Loss (gain) on insurance claims, legal finding and asset disposals | ( | ||||||||||||||||
| Change in operating assets and liabilities | |||||||||||||||||
| Accounts receivable | ( | ( | |||||||||||||||
| Prepaid income taxes | ( | ( | |||||||||||||||
| Prepaid expenses and other assets | ( | ( | ( | ||||||||||||||
| Deferred employer portion of social security taxes | ( | ( | |||||||||||||||
| Cash surrender value of life insurance policy premiums | ( | ( | ( | ||||||||||||||
| Deferred compensation liability | |||||||||||||||||
| Operating lease obligations | ( | ( | |||||||||||||||
| Accounts payable | |||||||||||||||||
| Accrued wages and related liabilities | |||||||||||||||||
| Other accrued liabilities | |||||||||||||||||
| Accrued self-insurance liabilities | |||||||||||||||||
| Other long-term liabilities | ( | ( | ( | ||||||||||||||
NET CASH PROVIDED BY OPERATING ACTIVITIES | $ | $ | $ | ||||||||||||||
| Cash flows from investing activities: | |||||||||||||||||
| Purchase of property and equipment | ( | ( | ( | ||||||||||||||
Cash payments for business acquisitions (Note 9) | ( | ( | |||||||||||||||
Cash payments for asset acquisitions (Note 9) | ( | ( | ( | ||||||||||||||
| Escrow deposits | ( | ||||||||||||||||
| Escrow deposits used to fund acquisitions | |||||||||||||||||
| Cash from insurance proceeds | |||||||||||||||||
| Cash proceeds from the sale of assets | |||||||||||||||||
| Deconsolidation of an ancillary business | ( | ||||||||||||||||
| Cash payments for Medicare and Medicaid licenses | ( | ||||||||||||||||
| Purchases of investments | ( | ( | ( | ||||||||||||||
| Maturities of investments | |||||||||||||||||
| Other restricted assets | ( | ( | |||||||||||||||
NET CASH USED IN INVESTING ACTIVITIES | $ | ( | $ | ( | $ | ( | |||||||||||
| Cash flows from financing activities: | |||||||||||||||||
Proceeds from debt (Note 16) | |||||||||||||||||
Payments on debt (Note 16) | ( | ( | ( | ||||||||||||||
| Issuance of common stock upon exercise of options | |||||||||||||||||
| Repurchase of shares of common stock to satisfy tax withholding obligations | ( | ( | ( | ||||||||||||||
Repurchase of shares of common stock (Note 22) | ( | ( | ( | ||||||||||||||
| Dividends paid | ( | ( | ( | ||||||||||||||
Proceeds from sale of subsidiary shares (Note 7) | |||||||||||||||||
| Non-controlling interest distribution | ( | ( | ( | ||||||||||||||
| Purchase of non-controlling interest | ( | ||||||||||||||||
| Payments of deferred financing costs | ( | ( | |||||||||||||||
Proceeds from CARES Act Provider Relief Fund and Medicare Advance Payment Program (Note 3) | |||||||||||||||||
Repayments of CARES Act Provider Relief Fund and Medicare Advance Payment Program (Note 3) | ( | ( | |||||||||||||||
NET CASH USED IN FINANCING ACTIVITIES | $ | ( | $ | ( | $ | ( | |||||||||||
| Net increase in cash and cash equivalents | |||||||||||||||||
| Cash and cash equivalents beginning of period | |||||||||||||||||
| Cash and cash equivalents end of period | $ | $ | $ | ||||||||||||||
| Year Ended December 31, | |||||||||||||||||
| (In thousands) | 2022 | 2021 | 2020 | ||||||||||||||
| SUPPLEMENTAL DISCLOSURES OF CASH FLOW INFORMATION | |||||||||||||||||
| Cash paid during the period for: | |||||||||||||||||
| Interest | $ | $ | $ | ||||||||||||||
| Income taxes | $ | $ | $ | ||||||||||||||
| Lease liabilities | $ | $ | $ | ||||||||||||||
| Non-cash financing and investing activity | |||||||||||||||||
| Accrued capital expenditures | $ | $ | $ | ||||||||||||||
| Accrued dividends declared | $ | $ | $ | ||||||||||||||
| Note receivable from insurance settlement | $ | $ | $ | ||||||||||||||
| Right-of-use assets obtained in exchange for new and modified operating lease obligations | $ | $ | $ | ||||||||||||||
See accompanying notes to consolidated financial statements.
95
THE ENSIGN GROUP, INC.
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS
(Dollars, shares and options in thousands, except per share data)
1. DESCRIPTION OF BUSINESS
The Company — The Ensign Group, Inc. (collectively, Ensign or the Company), is a holding company with no direct operating assets, employees or revenue. The Company's independent operating subsidiaries provide health care services across the post-acute care continuum, engaged in the ownership, acquisition, development and leasing of skilled nursing, senior living and other healthcare-related properties and other ancillary businesses. As of December 31, 2022, the Company's independent operating subsidiaries operated 271 facilities and other ancillary operations located in Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Nevada, South Carolina, Texas, Utah, Washington and Wisconsin. The Company's independent operating subsidiaries have a collective capacity of approximately 28,100 operational skilled nursing beds and 3,000 senior living units. As of December 31, 2022, the Company's independent operating subsidiaries operated 192 facilities under long-term lease arrangements, and had options to purchase 11 of those 192 facilities. The Company's real estate portfolio includes 108 owned real estate properties, which included 79 facilities operated and managed by the Company's independent operating subsidiaries, 29 senior living operations leased to and operated by The Pennant Group, Inc. (Pennant) as part of the spin-off transaction in October 2019, and the Service Center location. Of those 29 senior living operations, one is located on the same real estate property as a skilled nursing facility that the Company owns and operates.
Certain of the Company’s wholly-owned independent subsidiaries, collectively referred to as the Service Center, provide specific accounting, payroll, human resources, information technology, legal, risk management and other centralized services to the other operating subsidiaries through contractual relationships with such subsidiaries. The Company also has a wholly-owned captive insurance subsidiary that provides some claims-made coverage to the Company’s operating subsidiaries for general and professional liabilities, as well as coverage for certain workers’ compensation insurance liabilities.
In January of 2022, the Company formed a captive real estate investment trust (REIT), which owns and manages its real estate business, called Standard Bearer Healthcare REIT, Inc. (Standard Bearer). The Company expects the REIT structure will provide it with an efficient vehicle for future acquisitions of properties that could be operated by Ensign affiliates or other third parties. Refer to Note 7, Standard Bearer for additional information on Standard Bearer.
Each of the Company's affiliated operations are operated by separate, wholly-owned, independent subsidiaries that have their own management, employees and assets. References herein to the consolidated “Company” and “its” assets and activities in this Annual Report is not meant to imply, nor should it be construed as meaning that The Ensign Group, Inc. has direct operating assets, employees or revenue, or that any of the subsidiaries, are operated by The Ensign Group, Inc.
2. SUMMARY OF SIGNIFICANT ACCOUNTING POLICIES
96
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Insurance Subsidiary Deposits and Investments — The Company's captive insurance subsidiary cash and cash equivalents, deposits and investments are designated to support long-term insurance subsidiary liabilities and have been classified as short-term and long-term assets based on the timing of expected future payments of the Company's captive insurance liabilities. The majority of these deposits and investments are currently held in AA, A and BBB rated debt security investments and the remainder is held in a bank account with a high credit quality financial institution.
The Company's non-qualified deferred compensation plan (the DCP)'s contracts insuring the lives of certain employees who are eligible to participate in the DCP are held in a rabbi trust. Cash surrender value of the contracts is based on funds that shadow the investment allocations specified by participants in the deferred compensation plan. The fair value of the investment funds is derived using Level 2 inputs.
When evaluating an investment for its current expected credit losses, the Company reviews factors such as historical experience with defaults, losses, credit ratings, term, market sector and macroeconomic trends, including current conditions and forecasts to the extent they are reasonable and supportable.
97
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Leases and Leasehold Improvements — The Company leases skilled nursing facilities, senior living facilities and commercial office space. The Company determines if an arrangement is a lease at the inception of each lease. Leases commencing prior to the ASC 842 adoption date were classified as operating lease under historical guidance. As the Company has elected the package of practical expedients allowing it to not reassess lease classification, these leases are classified as operating leases under ASC 842 as well. For leases commencing subsequent to the ASC 842 adoption date, the Company performs an evaluation to determine whether the lease should be classified as an operating or finance lease at the inception of the lease. As of December 31, 2022, the Company does not have any leases that are classified as finance leases. Rights and obligations of operating leases are included as right-of-use assets, current lease liabilities and long-term lease liabilities on the Company's consolidated balance sheets. As the Company's leases do not provide an implicit rate, the Company uses its incremental borrowing rate based on the information available at lease commencement date in determining the present value of future lease payments. The Company utilized a third-party valuation specialist to assist in estimating the incremental borrowing rate.
The Company records rent expense for operating leases on a straight-line basis over the term of the lease. The lease term used for straight-line rent expense is calculated from the date the Company is given control of the leased premises through the end of the lease term. Renewals are not assumed in the determination of the lease term unless they are deemed to be reasonably assured at the inception of the lease. The lease term used for this evaluation also provides the basis for establishing depreciable lives for buildings subject to lease and leasehold improvements.
Intangible Assets and Goodwill — Definite-lived intangible assets consist primarily of patient base, facility trade names and customer relationships. Patient base is amortized over a period of to eight months , depending on the classification of the patients and the level of occupancy in a new acquisition on the acquisition date. Trade names at affiliated facilities are amortized over 30 years and customer relationships are amortized over a period of up to 20 years.
The Company's indefinite-lived intangible assets consist of trade names, and Medicare and Medicaid licenses. The Company tests indefinite-lived intangible assets for impairment on an annual basis or more frequently if events or changes in circumstances indicate that the carrying amount of the intangible asset may not be recoverable.
98
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Self-Insurance — The Company is partially self-insured for general and professional liability claims up to a base amount per claim (the self-insured retention) with an aggregate, one-time deductible above this limit. Losses beyond these amounts are insured through third-party policies with coverage limits per claim, per location and on an aggregate basis for the Company. The combined self-insured retention is $500 per claim, subject to an additional one-time deductible of $1,000 for California affiliated operations and a separate, one-time, deductible of $1,250 for non-California operations. For all affiliated operations, except those located in Colorado, the third-party coverage above these limits is $1,000 per claim, $3,000 per operation, with a $5,000 blanket aggregate limit and an additional state-specific aggregate where required by state law. In Colorado, the third-party coverage above these limits is $1,000 per claim and $3,000 per operation, which is independent of the aforementioned blanket aggregate limits that apply outside of Colorado.
The majority of the self-insured retention and deductible limits for general and professional liabilities and workers' compensation liabilities are self-insured through the captive insurance subsidiary, the related assets and liabilities of which are included in the accompanying consolidated balance sheets. The captive insurance subsidiary is subject to certain statutory requirements as an insurance provider.
The Company’s policy is to accrue amounts equal to the actuarial estimated costs to settle open claims of insureds, as well as an estimate of the cost of insured claims that have been incurred but not reported. The Company develops information about the size of the ultimate claims based on historical experience, current industry information and actuarial analysis, and evaluates the estimates for claim loss exposure on a quarterly basis. The Company uses actuarial valuations to estimate the liability based on historical experience and industry information.
The Company’s operating subsidiaries are self-insured for workers’ compensation liabilities in California. To protect itself against loss exposure in California with this policy, the Company has purchased individual specific excess insurance coverage that insures individual claims that exceed $625 per occurrence. In Texas, the operating subsidiaries have elected non-subscriber status for workers’ compensation claims and the Company has purchased individual stop-loss coverage that insures individual claims that exceed $750 per occurrence. The Company’s operating subsidiaries in all other states, with the exception of Washington, are under a loss sensitive plan that insures individual claims that exceed $350 per occurrence. In the state of Washington, the Company is self-insured and has purchased individual specific excess insurance coverage that insures individual claims that exceed $500 per occurrence. For all of the self-insured plans and retention, the Company accrues amounts equal to the estimated costs to settle open claims, as well as an estimate of the cost of claims that have been incurred but not reported. The Company uses actuarial valuations to estimate the liability based on historical experience and industry information.
In addition, the Company has recorded an asset and equal liability in order to present the ultimate costs of malpractice and workers' compensation claims and the anticipated insurance recoveries on a gross basis. See Note 13, Restricted and Other Assets.
The Company self-funds medical (including prescription drugs) and dental healthcare benefits to the majority of its employees. The Company is fully liable for all financial and legal aspects of these benefit plans. To protect itself against loss exposure with this policy, the Company has purchased individual stop-loss insurance coverage that insures individual claims that exceed $525 , $500 and $300 for each covered person for fiscal years 2022, 2021 and 2020, respectively.
The Company believes that adequate provision has been made in the Financial Statements for liabilities that may arise out of patient care, workers’ compensation, healthcare benefits and related services provided to date. The amount of the Company’s reserves was determined based on an estimation process that uses information obtained from both company-specific and industry data. This estimation process requires the Company to continuously monitor and evaluate the life cycle of the claims. Using data obtained from this monitoring and the Company’s assumptions about emerging trends, the Company, with the assistance of an independent actuary, develops information about the size of ultimate claims based on the Company’s historical experience and other available industry information. The most significant assumptions used in the estimation process include determining the trend in costs, the expected cost of claims incurred but not reported and the expected costs to settle or pay damage awards with respect to unpaid claims. The self-insured liabilities are based upon estimates, and while management believes that the estimates of loss are reasonable, the ultimate liability may be in excess of or less than the recorded amounts. Due to the inherent volatility of actuarially determined loss estimates, it is reasonably possible that the Company could experience changes in estimated losses that could be material to net income. If the Company’s actual liabilities exceed its estimates of losses, its future earnings, cash flows and financial condition would be adversely affected.
99
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Income Taxes — Deferred tax assets and liabilities are established for temporary differences between the financial reporting basis and the tax basis of the Company’s assets and liabilities at tax rates in effect when such temporary differences are expected to reverse. The Company generally expects to fully utilize its deferred tax assets; however, when necessary, the Company records a valuation allowance to reduce its net deferred tax assets to the amount that is more likely than not to be realized.
In determining the need for a valuation allowance or the need for and magnitude of liabilities for uncertain tax positions, the Company makes certain estimates and assumptions. These estimates and assumptions are based on, among other things, knowledge of operations, markets, historical trends and likely future changes and, when appropriate, the opinions of advisors with knowledge and expertise in certain fields. Due to certain risks associated with the Company’s estimates and assumptions, actual results could differ.
Recent Accounting Pronouncements — Except for rules and interpretive releases of the Securities and Exchange Commission (SEC) under authority of federal securities laws and a limited number of grandfathered standards, the FASB ASC is the sole source of authoritative GAAP literature recognized by the FASB and applicable to the Company. For any new pronouncements announced, the Company considers whether the new pronouncements could alter previous generally accepted accounting principles and determines whether any new or modified principles will have a material impact on the Company's reported financial position or operations in the near term. The applicability of any standard is subject to the formal review of the Company's financial management and certain standards are under consideration.
Recent Accounting Standards Adopted by the Company — In November 2021, the FASB issued ASU 2021-10 “Government Assistance (Topic 832): Disclosures by Business Entities about Government Assistance,” which created FASB ASC Topic 832, Government Assistance (ASC 832). ASC 832 requires business entities to disclose information about certain government assistance they receive. The Company adopted this standard on January 1, 2022 and determined there was no material impact on the Company's Financial Statements.
100
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
3. COVID-19 UPDATE
The COVID-19 pandemic has continued to impact the Company's affiliated operations. In prior years, as part of the Coronavirus Aid, Relief, and Economic Security Act of 2020 (the CARES Act), the Company received cash distributions of relief fund payments (Provider Relief Funds) and funds authorized by U.S. Department of Health and Human Services (HHS) to be used to protect residents of nursing homes and long-term care (LTC) facilities from the impact of COVID-19. During the year ended December 31, 2022, the Company did not receive Provider Relief Funds. During the year ended December 31, 2021 and 2020, the Company received and returned $11,637 and $141,700 , respectively, in Provider Relief Funds.
In fiscal year 2020, the Company applied for and received $105,255 through the Medicare Accelerated and Advance Payment Program under the CARES Act. The purpose of the program is to assist in providing needed liquidity to care delivery providers. The Company repaid $3,232 of the funds in 2020 and the remaining funds of $102,023 in March 2021.
The Families First Coronavirus Response Act was signed into law in 2020 to provide a temporary 6.2% increase to the Federal Medical Assistance Percentage (FMAP) effective January 1, 2020. The law permits states to retroactively change their state's Medicaid program rates effective as of January 1, 2020. The law provides discretion to each state and specifies the funds are to be used to reimburse the recipient for healthcare related expenses that are attributable to COVID-19 and associated with providing patient care. In addition, increases in Medicaid rates can come from other areas of the state's budget outside of FMAP funding. Revenues from these additional payments are recognized in accordance with ASC 606, subject to variable consideration constraints. In certain operations where the Company received additional payments that exceeded expenses incurred related to COVID-19, the Company characterized such payments as variable revenue that required additional consideration and accordingly, the amount of state relief revenue recognized is limited to the actual COVID-19 related expenses incurred. As of December 31, 2022 and 2021, the Company had $1,001 and $1,781 in unapplied state relief funds, respectively. During the years ended December 31, 2022, 2021, and 2020, the Company received an additional $81,057 , $70,484 , and $51,927 in state relief funding and recognized $81,837 , $75,231 , and $45,407 , respectively, as revenue.
The CARES Act also provides for deferred payment of the employer portion of social security taxes through the end of 2020, with approximately 50% of the deferred amount due by December 31, 2021 and the remaining 50% due by December 31, 2022. The Company recorded $48,309 of deferred payments of social security taxes as a liability during 2020, and paid the first and second half of the payments in the fourth quarters of 2021 and 2022, respectively.
4. REVENUE AND ACCOUNTS RECEIVABLE
Service Revenue
The Company's service revenue is derived primarily from providing healthcare services to its patients. Revenue is recognized when services are provided to the patients at the amount that reflects the consideration to which the Company expects to be entitled from patients and third-party payors, including Medicaid, Medicare and insurers (private and Medicare replacement plans), in exchange for providing patient care. The healthcare services in skilled patient contracts include routine services in exchange for a contractual agreed-upon amount or rate. Routine services are treated as a single performance obligation satisfied over time as services are rendered. As such, patient care services represent a bundle of services that are not capable of being distinct. Additionally, there may be ancillary services which are not included in the daily rates for routine services, but instead are treated as separate performance obligations satisfied at a point in time, if and when those services are rendered.
101
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Revenue recognized from healthcare services are adjusted for estimates of variable consideration to arrive at the transaction price. The Company determines the transaction price based on contractually agreed-upon amounts or rate on a per day basis, adjusted for estimates of variable consideration. The Company uses the expected value method in determining the variable component that should be used to arrive at the transaction price, using contractual agreements and historical reimbursement experience within each payor type. The amount of variable consideration which is included in the transaction price may be constrained, and is included in net revenue only to the extent that it is probable that a significant reversal in the amount of the cumulative revenue recognized will not occur in a future period. If actual amounts of consideration ultimately received differ from the Company’s estimates, the Company adjusts these estimates, which would affect net revenue in the period such variances become known.
Revenue from the Medicare and Medicaid programs accounted for 73.7 %, 73.6 % and 74.5 % for the years ended December 31, 2022, 2021, and 2020, respectively. Settlements with Medicare and Medicaid payors for retroactive adjustments due to audits and reviews are considered variable consideration and are included in the determination of the estimated transaction price. These settlements are estimated based on the terms of the payment agreement with the payor, correspondence from the payor and the Company’s historical settlement activity. Consistent with healthcare industry practices, any changes to these revenue estimates are recorded in the period the change or adjustment becomes known based on the final settlement. The Company recorded adjustments to revenue which were not material to the Company's revenue for the years ended December 31, 2022, 2021, and 2020.
Rental Revenue
The Company's rental revenues are primarily generated by leasing healthcare-related properties through triple-net lease arrangements, under which the tenant is solely responsible for the costs related to the property. Revenue is recognized on a straight-line basis over the lease term if it has been deemed probable of collection. The Company has elected the single component practical expedient, which allows a lessor, by class of underlying asset, not to allocate the total consideration to the lease and non-lease components based on their relative stand-alone selling prices where certain criteria are met.
Tenant reimbursements related to property taxes and insurance are neither considered lease nor non-lease components under the new lease standards. Lessee payments for taxes and insurance paid directly to a third party, on behalf of the Company, are excluded from variable lease payments and rental revenue in the Company’s consolidated statements of income. Otherwise, tenant reimbursements for taxes and insurance that are paid by the Company directly to a third party are classified as additional rental revenue and expense and recognized by the Company on a gross basis.
Disaggregation of Revenue
The Company disaggregates revenue from contracts with its patients by payors. The Company determines that disaggregating revenue into these categories achieves the disclosure objectives to depict how the nature, amount, timing and uncertainty of revenue and cash flows are affected by economic factors.
Revenue by Payor
The Company’s revenue is derived primarily from providing healthcare services to patients and is recognized on the date services are provided at amounts billable to individual patients, adjusted for estimates for variable consideration. For patients under reimbursement arrangements with third-party payors, including Medicaid, Medicare and private insurers, revenue is recorded based on contractually agreed-upon amounts or rates, adjusted for estimates for variable consideration, on a per patient, daily basis or as services are performed.
102
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Service revenue for the years ended December 31, 2022, 2021, and 2020 is summarized in the following tables:
| Year Ended December 31, | |||||||||||||||||||||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||||||||||||||||||||
| Revenue | % of Revenue | Revenue | % of Revenue | Revenue | % of Revenue | ||||||||||||||||||||||||||||||
Medicaid(1) | $ | % | $ | % | $ | % | |||||||||||||||||||||||||||||
| Medicare | |||||||||||||||||||||||||||||||||||
| Medicaid — skilled | |||||||||||||||||||||||||||||||||||
| Total Medicaid and Medicare | |||||||||||||||||||||||||||||||||||
| Managed care | |||||||||||||||||||||||||||||||||||
Private and other(2) | |||||||||||||||||||||||||||||||||||
| SERVICE REVENUE | $ | % | $ | % | $ | % | |||||||||||||||||||||||||||||
(2) Private and other payors also includes revenue from senior living operations and all payors generated in other ancillary services.
In addition to the service revenue above, the Company's rental revenue derived from triple-net lease arrangements with third parties is $16,757 , $15,985 and $15,157 for the years ended December 31, 2022, 2021, and 2020.
Balance Sheet Impact
Included in the Company’s consolidated balance sheets are contract balances, comprised of billed accounts receivable and unbilled receivables, which are the result of the timing of revenue recognition, billings and cash collections, as well as, contract liabilities, which primarily represent payments the Company receives in advance of services provided. The Company had no material contract liabilities and contract assets as of December 31, 2022 and 2021, or activity during the years ended December 31, 2022, 2021, and 2020.
Accounts receivable as of December 31, 2022 and 2021, is summarized in the following table:
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Medicaid | $ | $ | |||||||||
| Managed care | |||||||||||
| Medicare | |||||||||||
| Private and other payors | |||||||||||
| Less: allowance for doubtful accounts | ( | ( | |||||||||
| ACCOUNTS RECEIVABLE, NET | $ | $ | |||||||||
Practical Expedients and Exemptions
5. COMPUTATION OF NET INCOME PER COMMON SHARE
103
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
A reconciliation of the numerator and denominator used in the calculation of basic net income per common share follows:
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| NUMERATOR: | |||||||||||||||||
| Net income | $ | $ | $ | ||||||||||||||
| Less: net (loss) income attributable to noncontrolling interests | ( | ||||||||||||||||
| Net income attributable to The Ensign Group, Inc. | $ | $ | $ | ||||||||||||||
| DENOMINATOR: | |||||||||||||||||
| Weighted average shares outstanding for basic net income per share | |||||||||||||||||
| Basic net income per common share: | $ | $ | $ | ||||||||||||||
A reconciliation of the numerator and denominator used in the calculation of diluted net income per common share follows:
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| NUMERATOR: | |||||||||||||||||
| Net income | $ | $ | $ | ||||||||||||||
| Less: net (loss) income attributable to noncontrolling interests | ( | ||||||||||||||||
| Net income attributable to The Ensign Group, Inc. | $ | $ | $ | ||||||||||||||
| DENOMINATOR: | |||||||||||||||||
| Weighted average common shares outstanding | |||||||||||||||||
Plus: incremental shares from assumed conversion (1) | |||||||||||||||||
| Adjusted weighted average common shares outstanding | |||||||||||||||||
| Diluted net income per common share: | $ | $ | $ | ||||||||||||||
(1) Options outstanding which are anti-dilutive and therefore not factored into the weighted average common shares amount above were 780 , 198 and 956 for the years ended December 31, 2022, 2021 and 2020, respectively.
6. FAIR VALUE MEASUREMENTS
Fair value measurements are based on a three-tier hierarchy that prioritizes the inputs used to measure fair value. These tiers include: Level 1, defined as observable inputs such as quoted market prices in active markets; Level 2, defined as inputs other than quoted prices included within Level 1 that are observable for the asset or liability, either directly or indirectly; and Level 3, defined as unobservable inputs for which little or no market data exists, therefore requiring an entity to develop its own assumptions.
The fair value of cash and cash equivalents of $316,270 and $262,201 as of December 31, 2022 and 2021, respectively, is derived using Level 1 inputs. The Company's other financial assets include the captive insurance subsidiary's cash and cash equivalents, deposits and investments designated to support long-term insurance subsidiary liabilities and are carried at cost basis of $69,290 and $67,734 as of December 31, 2022 and 2021, respectively. Also included are contracts insuring the lives of certain employees who are eligible to participate in non-qualified deferred compensation plans which are held in a rabbi trust. The cash surrender value of these contracts is based on funds that shadow the investment allocations specified by participants in the deferred compensation plan. As of December 31, 2022, and 2021, the adjusted cost basis of the investment funds is $25,144 and $17,530 , respectively.
As of December 31, 2022 and 2021, the cost basis of the Company's financial assets included in the captive insurance subsidiary's investments and the deferred compensation plan investment funds are considered to approximate the fair value of these financial assets and are derived using Level 2 inputs.
104
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
7. STANDARD BEARER
Standard Bearer's real estate portfolio consists of 103 of the Company's 108 owned real estate properties, of which 75 are operated and managed by the Company and 29 are leased to and operated by Pennant. Of those 29 senior living operations, one is located on the same real estate property as a skilled nursing facility that the Company owns and operates. Standard Bearer intends to qualify and elect to be taxed as a REIT, for U.S. federal income tax purposes, commencing with its taxable year ended December 31, 2022. During the year ended December 31, 2022, Standard Bearer acquired the real estate of ten skilled nursing facilities for a purchase price of $84,656 , three of which were previously operated and managed by Ensign's affiliated operations. Refer to Note 9, Operation Expansions for additional information.
As part of the formation of Standard Bearer, certain of the Company's operating subsidiaries, Standard Bearer and Standard Bearer's subsidiaries entered into several agreements that include leasing, management services and debt arrangements between the operations. As these intercompany arrangements were entered into when Standard Bearer was formed in January 2022, the transactions related to these agreements are reflected in Standard Bearer's segment income during year ended December 31, 2022. All intercompany transactions have been eliminated in consolidation. Refer to Note 8, Business Segments, for additional information related to these intercompany eliminations as well as Standard Bearer as a reportable segment.
Intercompany master lease agreements
Certain of the Company's operating subsidiaries and the 75 Standard Bearer subsidiaries entered into five "triple-net" master lease agreements (collectively, the Standard Bearer Master Leases) in January 2022. The lease periods range from 15 to 19 years with three five-year renewal options beyond the initial term, on the same terms and conditions. The rent structure under the Standard Bearer Master Leases includes a fixed component, subject to annual escalation equal to the lesser of (1) the percentage change in the Consumer Price Index (but not less than zero ) or (2) 2.5 %. In addition to rent, the operating subsidiaries are required to pay the following: (1) all impositions and taxes levied on or with respect to the leased properties; (2) all utilities and other services necessary or appropriate for the leased properties and the business conducted on the leased properties; (3) all insurance required in connection with the leased properties and the business conducted on the leased properties; (4) all facility maintenance and repair costs; and (5) all fees in connection with any licenses or authorizations necessary or appropriate for the leased properties and the business conducted on the leased properties. The ten real estate properties acquired during year ended December 31, 2022 were added to the Standard Bearer Master Leases. Rental revenue generated from Ensign affiliated operations was $57,967 , $44,165 and $40,946 for the years ended December 31, 2022, 2021, and 2020, respectively. As of December 31, 2022, total annual rental income under the Standard Bearer Master Lease is approximately $62.5 million.
Intercompany management agreement
Standard Bearer has no employees. The Service Center provides personnel and services to Standard Bearer pursuant to the management agreement between Standard Bearer and the Service Center. The management agreement provides for a base management fee that is equal to 5 % of total rental revenue and an incentive management fee that is equal to 5 % of funds from operations (FFO) and is capped at 1 % of total rental revenue. Management fee generated between Standard Bearer and the Service Center for the year ended December 31, 2022 was $4,367 , which represents 6 No
Intercompany debt arrangements
Standard Bearer obtains its funding through various sources including operating cash flows, access to debt arrangements and intercompany loans. The intercompany debt arrangements include mortgage loans and the Revolving Credit Facility to fund acquisitions and working capital needs. The interest rate under the Amended Credit Agreement is a base rate plus a margin ranging from 0.25 % to 1.25 % per annum or SOFR plus a margin range from 1.25 % to 2.25 % per annum.
105
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
In addition, as the Department of Housing and Urban Development (HUD) mortgage loans and promissory notes are entered into by real estate subsidiaries of Standard Bearer, the interest expense incurred from these debts are included in Standard Bearer's segment income. Refer to Note 16, Debt, for additional information related to these debts.
Equity Instrument Denominated in the Shares of a Subsidiary
As part of the formation of Standard Bearer in January of 2022, the Company established the Standard Bearer Healthcare REIT, Inc. 2022 Omnibus Incentive Plan (Standard Bearer Equity Plan). The Company may grant stock options and restricted stock awards under the Standard Bearer Equity Plan to employees and management of Ensign's affiliated subsidiaries. These awards generally vest over a period of five years or upon the occurrence of certain prescribed events. The value of the stock options and restricted stock awards is tied to the value of the common stock of Standard Bearer, which is determined based on an independent valuation of Standard Bearer. The awards can be put to Standard Bearer at various prescribed dates, which in no event is earlier than six months after vesting of the restricted awards or exercise of the stock options. The Company can also call the awards, generally upon employee termination. During the year ended December 31, 2022, Standard Bearer sold fully vested common shares from the Standard Bearer Equity Plan to shareholders for cash of $6,544 . During the year ended December 31, 2022, the Company did not
During the year ended December 31, 2022, Standard Bearer established shareholders of its preferred shares through contributions of cash of $149 . These preferred shares were fully vested at the time of the contributions by the shareholders. The value of Standard Bearer common and preferred shares held by the Company are eliminated in consolidation and the value held by other shareholders are classified as noncontrolling interests on the Company's consolidated balance sheets.
Dividends on Shares of a Subsidiary
During the year ended December 31, 2022, Standard Bearer met the requirement to distribute to its shareholders at least 90% of its annual taxable income through a declaration and payment of cash dividends totaling $30,379 . Of that amount, $30,095 was paid in the form of a distribution to the Company and $284 was paid in the form of a distribution to noncontrolling interests.
8. BUSINESS SEGMENTS
In conjunction with the formation of Standard Bearer in January 2022, the Company's Chief Executive Officer, who is its chief operating decision maker, or CODM, began reviewing the results of Standard Bearer instead of all real estate properties. Accordingly, the Company revised its former real estate segment to include only real estate properties that are part of Standard Bearer. This change in organizational structure demonstrates that Standard Bearer's real estate is a core part of the Company's expansion of its real estate investment strategy. As of the first quarter of 2022, the Company has two reportable segments: (1) skilled services, which includes the operation of skilled nursing facilities and rehabilitation therapy services and (2) Standard Bearer, which is comprised of selected real estate properties owned by Standard Bearer and leased to skilled nursing and senior living operators. Segment information for prior periods has been recast to reflect the change of the Company’s segment structure.
As of December 31, 2022, the skilled services segment includes 234 skilled nursing operations and 26 campus operations that provide both skilled nursing and rehabilitative care services and senior living services. The Company's Standard Bearer segment consists of 103 owned real estate properties. These properties include 75 operations the Company operated and managed and 29 senior living operations that are leased to and operated by third parties. Of the 29 real estate operations leased to third parties, one senior living operation is located on the same real estate property as a skilled nursing facility that the Company owns and operates.
The Company also reports an “All Other” category that includes results from its senior living operations, which includes eleven stand-alone senior living operations and the senior living operations at 26 campus operations that provide both skilled nursing and rehabilitative care services and senior living services. In addition, the "All Other" category includes mobile diagnostics, medical transportation, other real estate and other ancillary operations. Services included in the “All Other” category are insignificant individually, and therefore do not constitute a reportable segment.
106
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
The Company’s reportable segments are significant operating segments that offer differentiated services. The Company's CODM reviews financial information for each operating segment to evaluate performance and allocate capital resources. This structure reflects its current operational and financial management and provides the best structure to maximize the quality of care and investment strategy provided, while maintaining financial discipline. The Company's CODM does not review assets by segment in his resource allocation and therefore assets by segment are not disclosed below.
The accounting policies of the reportable segments are the same as those described in Note 2, Summary of Significant Accounting Policies. Intercompany revenue is eliminated in consolidation, along with corresponding intercompany expenses. Segment income and loss is defined as profit or loss from operations before provision for income taxes, excluding gain or loss from sale of real estate, real estate insurance recoveries and losses and impairment charges from operations. Included in segment income for Standard Bearer is expense for intercompany services provided by the Service Center as described in Note 7, Standard Bearer, as it is part of the CODM financial information.
The following tables set forth financial information for the segments:
| Year Ended December 31, 2022 | ||||||||||||||||||||||||||||||||
| Skilled Services | Standard Bearer | All Other(1) | Intercompany Elimination | Total | ||||||||||||||||||||||||||||
Service revenue(2) | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
Rental revenue(3) | ( | |||||||||||||||||||||||||||||||
| TOTAL REVENUE | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
| Segment income (loss) | ( | |||||||||||||||||||||||||||||||
| Gain on sale of real estate assets and insurance recoveries, net | ||||||||||||||||||||||||||||||||
| Income before provision for income taxes | $ | |||||||||||||||||||||||||||||||
| Depreciation and amortization | ||||||||||||||||||||||||||||||||
Interest expense(4) | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
(1) All other primarily includes all ancillary operations, stand-alone senior living operations and the Service Center.
(2) Intercompany service revenue represents service revenue generated by ancillary operations provided to the Company's affiliated wholly-owned healthcare facilities and management service revenue generated by the Service Center with Standard Bearer. Intercompany service revenue is eliminated in consolidation along with corresponding intercompany cost of service.
(3) Intercompany rental revenue represents rental income generated by both Standard Bearer and other real estate properties with the Company's affiliated wholly-owned healthcare facilities. Intercompany rental revenue is eliminated in consolidation along with corresponding intercompany rent expense.
(4) Included in interest expense in Standard Bearer is interest expense incurred from intercompany debt arrangements between Standard Bearer and The Ensign Group, Inc. The intercompany interest expense is eliminated in the "Intercompany Elimination" column.
| Year Ended December 31, 2021 | ||||||||||||||||||||||||||||||||
| Skilled Services | Standard Bearer | All Other(1) | Intercompany Elimination | Total | ||||||||||||||||||||||||||||
Service revenue(2) | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
Rental revenue(3) | ( | |||||||||||||||||||||||||||||||
| TOTAL REVENUE | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
| Segment income (loss) | ( | |||||||||||||||||||||||||||||||
| Gain on real estate insurance recoveries | ||||||||||||||||||||||||||||||||
| Income before provision for income taxes | $ | |||||||||||||||||||||||||||||||
| Depreciation and amortization | ||||||||||||||||||||||||||||||||
| Interest expense | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||
(1) All other primarily includes all ancillary operations, stand-alone senior living operations and the Service Center.
(2) Intercompany service revenue represents service revenue generated by ancillary operations provided to the Company's affiliated wholly-owned healthcare facilities. Intercompany service revenue is eliminated in consolidation along with corresponding intercompany cost of service.
(3) Intercompany rental revenue represents rental income generated by both Standard Bearer and other real estate properties with the Company's affiliated wholly-owned healthcare facilities. Intercompany rental revenue is eliminated in consolidation along with corresponding intercompany rent expense.
107
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Year Ended December 31, 2020 | ||||||||||||||||||||||||||||||||
| Skilled Services | Standard Bearer | All Other(1) | Intercompany Elimination | Total | ||||||||||||||||||||||||||||
Service revenue(2) | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
Rental revenue(3) | ( | |||||||||||||||||||||||||||||||
| TOTAL REVENUE | $ | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||
| Segment income (loss) | ( | |||||||||||||||||||||||||||||||
| Loss on sale of real estate and impairment charges | ( | |||||||||||||||||||||||||||||||
| Income before provision for income taxes | $ | |||||||||||||||||||||||||||||||
| Depreciation and amortization | ||||||||||||||||||||||||||||||||
| Interest expense | $ | $ | $ | $ | $ | |||||||||||||||||||||||||||
(1) All other primarily includes all ancillary operations, stand-alone senior living operations and the Service Center.
(2) Intercompany service revenue represents service revenue generated by ancillary operations provided to the Company's affiliated wholly-owned healthcare facilities. Intercompany service revenue is eliminated in consolidation along with corresponding intercompany cost of service.
Service revenue by major payor source were as follows:
| Year Ended December 31, 2022 | ||||||||||||||||||||||||||
| Skilled Services | Other Service Revenue | Total Service Revenue | Revenue % | |||||||||||||||||||||||
Medicaid(1) | $ | $ | $ | % | ||||||||||||||||||||||
| Medicare | ||||||||||||||||||||||||||
| Medicaid-skilled | ||||||||||||||||||||||||||
| Subtotal | ||||||||||||||||||||||||||
| Managed care | ||||||||||||||||||||||||||
Private and other(2) | ||||||||||||||||||||||||||
| TOTAL SERVICE REVENUE | $ | $ | $ | % | ||||||||||||||||||||||
(1) Medicaid payor includes revenue generated from senior living operations and revenue related to FMAP and other COVID-19 related state funding.
(2) Private and other payors also includes revenue from senior living operations and all payors generated in other ancillary services.
| Year Ended December 31, 2021 | ||||||||||||||||||||||||||
| Skilled Services | Other Service Revenue | Total Service Revenue | Revenue % | |||||||||||||||||||||||
Medicaid(1) | $ | $ | $ | % | ||||||||||||||||||||||
| Medicare | ||||||||||||||||||||||||||
| Medicaid-skilled | ||||||||||||||||||||||||||
| Subtotal | ||||||||||||||||||||||||||
| Managed care | ||||||||||||||||||||||||||
Private and other(2) | ||||||||||||||||||||||||||
| TOTAL SERVICE REVENUE | $ | $ | $ | % | ||||||||||||||||||||||
(1) Medicaid payor includes revenue generated from senior living operations and revenue related to FMAP and other COVID-19 related state funding.
(2) Private and other payors also includes revenue from senior living operations and all payors generated in other ancillary services.
108
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Year Ended December 31, 2020 | ||||||||||||||||||||||||||
| Skilled Services | Other Service Revenue | Total Service Revenue | Revenue % | |||||||||||||||||||||||
Medicaid(1) | $ | $ | $ | % | ||||||||||||||||||||||
| Medicare | ||||||||||||||||||||||||||
| Medicaid-skilled | ||||||||||||||||||||||||||
| Subtotal | ||||||||||||||||||||||||||
| Managed care | ||||||||||||||||||||||||||
Private and other(2) | ||||||||||||||||||||||||||
| TOTAL SERVICE REVENUE | $ | $ | $ | % | ||||||||||||||||||||||
(1) Medicaid payor includes revenue generated from senior living operations and revenue related to FMAP and other COVID-19 related state funding.
(2) Private and other payors also includes revenue from senior living operations and all payors generated in other ancillary services.
9. OPERATION EXPANSIONS
The Company's subsidiaries expansion focus is to purchase or lease operations that are complementary to the current affiliated operations, accretive to the business, or otherwise advance the Company's strategy. The results of all operating subsidiaries are included in the Financial Statements subsequent to the date of acquisition. Acquisitions are accounted for using the acquisition method of accounting. The Company's affiliated operations also enter into long-term leases that may include options to purchase the facilities. As a result, from time to time, a real estate affiliated subsidiary will acquire the property of facilities that have previously been operated under third-party leases.
FASB ASC Topic 805, Clarifying the Definition of a Business (ASC 805) defined the definition of a business to assist entities with evaluating when a set of transferred assets and activities is deemed to be a business. Determining whether a transferred set constitutes a business is important because the accounting for a business combination differs from that of an asset acquisition. The definition of a business also affects the accounting for dispositions. When substantially all of the fair value of assets acquired is concentrated in a single asset, or a group of similar assets, the assets acquired would not represent a business and business combination accounting would not be required.
2022 Expansions
During the year ended December 31, 2022, the Company expanded its operations through a combination of long-term leases and real estate purchases, with the addition of 23 stand-alone skilled nursing operations and one campus operation. Of these additions, Standard Bearer acquired the real estate of seven of the stand-alone skilled nursing operations, which were leased back to Ensign affiliated entities. In addition, the Company purchased the real estate at three skilled nursing properties that the Company was already operating, further expanding the Company's real estate portfolio. Refer to Note 7, Standard Bearer, for additional information on the purchase of real estate properties. In addition, the Company added five senior living operations that were transferred from Pennant, three of which are part of campuses operated by the Company's affiliated operating subsidiaries. These new operations added a total of 3,058 operational skilled nursing beds and 674 operational senior living units to be operated by the Company's affiliated operating subsidiaries. The Company also invested in new ancillary services that are complementary to its existing businesses. The aggregate purchase price for these expansions during the year ended December 31, 2022 was $101,136 .
In connection with the new operations made through long-term leases, the Company did not acquire any material assets or assume any liabilities other than the tenant's post-assumption rights and obligations under the long-term lease. The Company entered into a separate operations transfer agreement with the prior operator as part of each transaction.
The aggregate purchase price for the transactions that were classified as asset acquisitions during the year ended December 31, 2022 was $84,736 , consisting of real estate properties and indefinite-lived intangible assets. The remaining aggregate purchase price for transactions during the year ended December 31, 2022 was concentrated in goodwill of $16,400 and accordingly, the transactions were classified as business combinations.
Subsequent to December 31, 2022, the Company expanded its operations through a combination of long-term leases, with the addition of seventeen stand-alone skilled nursing operations. These new operations added 1,462 operational skilled nursing beds. The Company also invested in new ancillary services that are complementary to its existing businesses. In connection with the new operations made through long-term leases, the Company did not acquire any material assets or assume any liabilities other than the tenant's post-assumption rights and obligations under the long-term lease. The Company entered into a separate operations transfer agreement with the prior operator as part of each transaction.
109
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
2021 Expansions
During the year ended December 31, 2021, the Company expanded its operations through a combination of long-term leases and a real estate purchase, with the addition of 17 stand-alone skilled nursing operations and five real estate purchases, four of which the Company previously operated and continues to operate. The remaining real estate purchase is operated by Pennant. These new operations added a total of 1,832 operational skilled nursing beds operated by the Company's affiliated operating subsidiaries. The aggregate purchase price for these acquisitions during the year ended December 31, 2021 was $104,224 .
In connection with the new operations made through long-term leases, the Company did not acquire any material assets or assume any liabilities other than the tenant's post-assumption rights and obligations under the long-term lease. The Company entered into a separate operations transfer agreement with the prior operator as part of each transaction.
The aggregate purchase price for the asset acquisitions during the year ended December 31, 2021 was $98,224 , consisting of real estate properties. The fair value of assets for the remaining additions was concentrated in goodwill of $6,000 and as such, the transaction was classified as a business combination.
2020 Acquisitions
During the year ended December 31, 2020, the Company expanded its operations through a combination of long-term leases and real estate purchases, with the addition of five stand-alone skilled nursing operations, one stand-alone senior living operation and one campus operation. Of these additions, four are related to purchases of owned properties, further expanding the Company's real estate portfolio. These new operations added a total of 507 operational skilled nursing beds and 298 operational senior living units to be operated by the Company's affiliated operating subsidiaries. The aggregate purchase price for these acquisitions during the year ended December 31, 2020 was $24,997 .
In connection with the new operations made through long-term leases, the Company did not acquire any material assets or assume any liabilities other than the tenant's post-assumption rights and obligations under the long-term lease. The Company entered into a separate operations transfer agreement with the prior operator as part of each transaction.
The fair value of assets for the purchases of these properties was concentrated in property and equipment and as such, these transactions were classified as asset acquisitions.
During the first quarter of 2020, the Company entered into a long-term lease agreement to transfer two senior living operations to Pennant. Ensign affiliates retained ownership of the real estate for these two senior living communities, which was subsequently sold in 2022.
The table below presents the allocation of the purchase price for the operations acquired during the years ended December 31, 2022, 2021, and 2020, excluding assets that were contributed to Pennant that occurred during the spin-off transaction in 2019.
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| Land | $ | $ | $ | ||||||||||||||
| Building and improvements | |||||||||||||||||
| Equipment, furniture, and fixtures | |||||||||||||||||
| Assembled occupancy | |||||||||||||||||
| Goodwill | |||||||||||||||||
| Leased asset | |||||||||||||||||
| Other indefinite-lived intangible assets | |||||||||||||||||
| TOTAL ACQUISITIONS | $ | $ | $ | ||||||||||||||
110
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
10. PROPERTY AND EQUIPMENT - NET
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Land | $ | $ | |||||||||
| Buildings and improvements | |||||||||||
| Leasehold improvements | |||||||||||
| Equipment | |||||||||||
| Furniture and fixtures | |||||||||||
| Construction in progress | |||||||||||
| Less: accumulated depreciation | ( | ( | |||||||||
| PROPERTY AND EQUIPMENT, NET | $ | $ | |||||||||
The Company completed the sale of assets for a sale price of $8,607 and recorded a gain of $3,467 within the Company's consolidated statement of income as cost of services during the year ended December 31, 2022. In addition, the Company evaluated its long-lived assets and did not impairment charges of $2,681 for the fiscal year ended 2020. See also Note 7, Standard Bearer and Note 9, Operation Expansions for information on acquisitions during the year ended December 31, 2022.
11. INTANGIBLE ASSETS - NET
| Weighted Average Life (Years) | December 31, | |||||||||||||||||||||||||||||||||||||||||||
| 2022 | 2021 | |||||||||||||||||||||||||||||||||||||||||||
| Gross Carrying Amount | Accumulated Amortization | Gross Carrying Amount | Accumulated Amortization | |||||||||||||||||||||||||||||||||||||||||
| Intangible Assets | Net | Net | ||||||||||||||||||||||||||||||||||||||||||
| Assembled occupancy | $ | $ | ( | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||||||||||||
| Facility trade name | ( | ( | ||||||||||||||||||||||||||||||||||||||||||
| Customer relationships | ( | ( | ||||||||||||||||||||||||||||||||||||||||||
| TOTAL | $ | $ | ( | $ | $ | $ | ( | $ | ||||||||||||||||||||||||||||||||||||
During the years ended December 31, 2022, 2021, and 2020, amortization expense was $1,714 , $1,435 and $1,813 , respectively, of which $1,160 , $1,158 , and $1,223 was related to the amortization of right-of-use assets, respectively. The Company did not
111
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
| Year | Amount | |||||||
| 2023 | $ | |||||||
| 2024 | ||||||||
| 2025 | ||||||||
| 2026 | ||||||||
| 2027 | ||||||||
| Thereafter | ||||||||
| $ | ||||||||
12. GOODWILL AND OTHER INDEFINITE-LIVED INTANGIBLE ASSETS
The Company tests goodwill during the fourth quarter of each year or more often if events or circumstances indicate there may be impairment. The Company performs its analysis for each reporting unit that constitutes a business for which discrete financial information is produced and reviewed by operating segment management and provides services that are distinct from the other components of the operating segment, in accordance with the provisions of FASB ASC Topic 350, Intangibles—Goodwill and Other (ASC 350). This guidance provides the option to first assess qualitative factors to determine whether it is more likely than not that the fair value of a reporting unit is less than its carrying value. If, based on a review of qualitative factors, it is more likely than not that the fair value of a reporting unit is less than its carrying value, the Company performs a goodwill impairment test by comparing the carrying value of each reporting unit to its respective fair value. The Company determines the estimated fair value of each reporting unit using a discounted cash flow analysis. The fair value of the reporting unit is the implied fair value of goodwill. In the event a reporting unit's carrying value exceeds its fair value, an impairment loss will be recognized. An impairment loss is measured by the difference between the carrying value of the reporting unit and its fair value.
The Company performs its goodwill impairment test annually and evaluates goodwill when events or changes in circumstances indicate that its carrying value may not be recoverable. The Company performs the annual impairment testing of goodwill using October 1 as the measurement date. The Company completed its goodwill impairment test as of October 1, 2022 and did no 7,410 .
The Company anticipates that the majority of goodwill recognized will be fully deductible for tax purposes as of December 31, 2022.
All of the Company's acquisitions during the year ended December 31, 2020 were classified as asset acquisitions and accordingly, no goodwill was recognized for these acquisitions. There were no other activities in goodwill during the year ended December 31, 2020. Provided that goodwill corresponds to the acquisition of a business and not merely the acquisition of real estate property, the Company's Standard Bearer segment appropriately does not carry a goodwill balance. The following table represents activity in goodwill by skilled service segment and "all other" category as of and for the year ended December 31, 2022, 2021 and 2020:
| Goodwill | |||||||||||||||||
| Skilled Services | All Other | Total | |||||||||||||||
| January 1, 2020 | $ | $ | $ | ||||||||||||||
| December 31, 2020 | $ | $ | $ | ||||||||||||||
| Additions | |||||||||||||||||
| December 31, 2021 | $ | $ | $ | ||||||||||||||
| Additions | |||||||||||||||||
| December 31, 2022 | $ | $ | $ | ||||||||||||||
During the year ended December 31, 2022, the Company acquired $245 in Medicare and Medicaid licenses compared to $181 and $648 in the fiscal years 2021 and 2020, respectively.
112
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Other indefinite-lived intangible assets consist of the following:
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Trade name | $ | $ | |||||||||
| Medicare and Medicaid licenses | |||||||||||
| TOTAL | $ | $ | |||||||||
13. RESTRICTED AND OTHER ASSETS
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Debt issuance costs, net | $ | $ | |||||||||
| Long-term insurance losses recoverable asset | |||||||||||
| Capital improvement reserves with landlords and lenders | |||||||||||
| Deposits with landlords | |||||||||||
| Other | |||||||||||
| RESTRICTED AND OTHER ASSETS | $ | $ | |||||||||
14. OTHER ACCRUED LIABILITIES
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Quality assurance fee | $ | $ | |||||||||
| Refunds payable | |||||||||||
| Resident advances | |||||||||||
| Unapplied state relief funds | |||||||||||
| Cash held in trust for patients | |||||||||||
| Dividends payable | |||||||||||
| Property taxes | |||||||||||
| Legal finding accrued | |||||||||||
| Other | |||||||||||
| OTHER ACCRUED LIABILITIES | $ | $ | |||||||||
Quality assurance fee represents the aggregate of amounts payable to Arizona, California, Colorado, Idaho, Iowa, Kansas, Nebraska, Nevada, Utah, Washington and Wisconsin as a result of a mandated fee based on patient days or licensed beds. Refunds payable includes payables related to overpayments, duplicate payments and credit balances from various payor sources. Resident advances occur when the Company receives payments in advance of services provided. Cash held in trust for patients reflects monies received from or on behalf of patients. Maintaining a trust account for patients is a regulatory requirement and, while the trust assets offset the liabilities, the Company assumes a fiduciary responsibility for these funds. The cash balance related to this liability is included in other current assets in the consolidated balance sheets.
113
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
15. INCOME TAXES
The provision for income taxes on continuing operations for the years ended December 31, 2022, 2021 and 2020 is summarized as follows:
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| Current: | |||||||||||||||||
| Federal | $ | $ | $ | ||||||||||||||
| State | |||||||||||||||||
| Deferred: | |||||||||||||||||
| Federal | ( | ( | ( | ||||||||||||||
| State | ( | ( | ( | ||||||||||||||
| ( | ( | ( | |||||||||||||||
| TOTAL | $ | $ | $ | ||||||||||||||
A reconciliation of the federal statutory rate to the effective tax rate for income from continuing operations for the years ended December 31, 2022, 2021 and 2020, respectively, is comprised as follows:
| December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| Income tax expense at statutory rate | % | % | % | ||||||||||||||
| State income taxes - net of federal benefit | |||||||||||||||||
| Non-deductible expenses | |||||||||||||||||
| Equity compensation | ( | ( | ( | ||||||||||||||
| Other adjustments | ( | ( | ( | ||||||||||||||
| TOTAL INCOME TAX PROVISION | % | % | % | ||||||||||||||
The Company's effective tax rate was 22.3 % for the year ended December 31, 2022, compared to 23.4 % for the same period in 2021 and 21.3 % in 2020. The lower effective tax rate is due to higher tax benefits from stock compensation and lower tax expense from non-deductible expenses.
114
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
The Company's deferred tax assets and liabilities as of December 31, 2022 and 2021 are summarized below.
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Deferred tax assets (liabilities): | |||||||||||
| Accrued expenses | $ | $ | |||||||||
| Revenue related reserves | |||||||||||
| Tax credits | |||||||||||
| Insurance | |||||||||||
| Lease liability | |||||||||||
| State taxes | ( | ||||||||||
| Valuation allowance | ( | ( | |||||||||
| TOTAL DEFERRED TAX ASSETS | |||||||||||
| Depreciation and amortization | ( | ( | |||||||||
| Prepaid expenses | ( | ( | |||||||||
| Right of use asset | ( | ( | |||||||||
| TOTAL DEFERRED TAX LIABILITIES | ( | ( | |||||||||
| NET DEFERRED TAX ASSETS | $ | $ | |||||||||
The Company had state credit carryforwards as of December 31, 2022 and 2021 of $1,742 and $2,138 , respectively. These carryforwards almost entirely relate to state limitations on the application of Enterprise Zone employment-related tax credits. Unless the Company uses the Enterprise Zone credits beforehand, the carryforward will begin to expire in 2023. As of December 31, 2022 and 2021, the valuation allowance of $789
The Company's operating loss carry forwards for states were not material during the years ended December 31, 2022 and 2021.
As of December 31, 2022, 2021 and 2020, the Company did not have any unrecognized tax benefits, net of its state benefits that would affect the Company's effective tax rate. The Company classifies interest and/or penalties on income tax liabilities or refunds as additional income tax expense or income. Such amounts are not material.
The Federal statutes of limitations on the Company's 2018, 2017, and 2016 income tax years lapsed during the third quarter of 2022, 2021, and 2020, respectively. During the fourth quarter of each year, various state statutes of limitations also lapsed. The lapses for the years ended December 31, 2022 and 2021 had no impact on the Company's unrecognized tax benefits.
During the year ended December 31, 2021, the state of Wisconsin initiated and completed an examination of the Company's 2019, 2018, and 2017 state tax years with no adjustments. The Company is not under examination by any major income tax jurisdiction.
16. DEBT
Debt consists of the following:
| December 31, | |||||||||||
| 2022 | 2021 | ||||||||||
| Mortgage loans and promissory notes | $ | $ | |||||||||
| Less: current maturities | ( | ( | |||||||||
| Less: debt issuance costs, net | ( | ( | |||||||||
| LONG-TERM DEBT LESS CURRENT MATURITIES | $ | $ | |||||||||
115
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Credit Facility with a Lending Consortium Arranged by Truist
The Company maintains a revolving credit facility between the Company and its subsidiaries, including Standard Bearer as co-borrowers, and Truist Securities (Truist) (the Revolving Credit Facility). Borrowings are supported by a lending consortium arranged by Truist. On April 8, 2022, the Company and its subsidiaries, including Standard Bearer, entered into the Amended Credit Agreement, which amended the Revolving Credit Facility to increase the revolving line of credit from $350,000 to $600,000 in aggregate principal amount. The Amended Credit Agreement also extended the maturity date of the Revolving Credit Facility to April 8, 2027 and modified the reference rate from LIBOR to SOFR. The interest rates applicable to loans under the Amended Credit Facility are, at the Company's option, equal to either a base rate plus a margin ranging from 0.25 % to 1.25 % per annum or SOFR plus a margin range from 1.25 % to 2.25 % per annum, based on the Consolidated Total Net Debt to Consolidated EBITDA ratio (as defined in the agreement). In addition, the Company and its subsidiaries, including Standard Bearer, will pay a commitment fee on the unused portion of the commitments that will range from 0.20 % to 0.40 % per annum, depending on the Consolidated Total Net Debt to Consolidated EBITDA ratio. Except as set forth in the Amended Credit Facility, all other terms and conditions of the Credit Facility remained in full force and effect as described below. As part of the entry into the Amended Credit Agreement, deferred financing costs of $566 were written off and additional deferred financing costs of $3,197 were capitalized during the year ended December 31, 2022.
Borrowings made under the Revolving Credit Facility are guaranteed, jointly and severally, by certain of the Company’s wholly-owned subsidiaries, and are secured by a pledge of stock of the Company's material operating subsidiaries as well as a first lien on substantially all of their personal property. The Amended Credit Agreement contains customary covenants that, among other things, restrict, subject to certain exceptions, the ability of the Company and its operating subsidiaries to grant liens on their assets, incur indebtedness, sell assets, make investments, engage in acquisitions, mergers or consolidations, amend certain material agreements and pay certain dividends and other restricted payments. Under the Amended Credit Agreement, the Company must comply with financial maintenance covenants to be tested quarterly, consisting of (i) a maximum consolidated total net debt to consolidated EBITDA ratio (which shall not be greater than 3.00 :1.00; provided that if the aggregate consideration for approved acquisitions in a six months period is greater than $50,000 , then the ratio can be increased at the election of the Company with notice to the administrative agent to 3.50 :1.00 for the first fiscal quarter and the immediately following three fiscal quarters), and (ii) a minimum interest/rent coverage ratio (which cannot be less than 1.50 :1.00). As of December 31, 2022, and January 30, 2023, there was no
Mortgage Loans and Promissory Notes
As of December 31, 2022, the Company's operating subsidiaries had $156,271 outstanding under the mortgage loans and notes, of which $3,883 is classified as short-term and the remaining $152,388 is classified as long-term. The Company was in compliance with all loan covenants as of December 31, 2022.
As of December 31, 2022, 23 of the Company's subsidiaries have mortgage loans insured with HUD in the aggregate amount of $153,488 , which subjects these subsidiaries to HUD oversight and periodic inspections. The mortgage loans bear effective interest rates in a range of 3.1 % to 4.2 %, including fixed interest rates in a range of 2.4 % to 3.3 % per annum. In addition to the interest rate, we incur other fees for HUD placement, including but not limited to audit fees. Amounts borrowed under the mortgage loans may be prepaid, subject to prepayment fees based on the principal balance on the date of prepayment. For the majority of the loans, during the first three years , the prepayment fee is 10.0 % and is reduced by 3.0 % in the fourth year of the loan, and reduced by 1.0 % per year for years through of the loan. There is no prepayment penalty after year . The terms for all the mortgage loans are 25 to 35 years.
In addition to the HUD mortgage loans above, the Company has two promissory notes. The notes bear fixed interest rates of 6.3 % and 5.3 % per annum and the term of the notes are 10 months and 12 years, respectively. The 12 year note which was used for an acquisition is secured by the real property comprising the facility and the rent, issues and profits thereof, as well as all personal property used in the operation of the facility.
116
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Future principal payments due under the long-term debt arrangements discussed above are as follows:
| Years Ending December 31, | Amount | |||||||
| 2023 | $ | |||||||
| 2024 | ||||||||
| 2025 | ||||||||
| 2026 | ||||||||
| 2027 | ||||||||
| Thereafter | ||||||||
| $ | ||||||||
Based on Level 2, the carrying value of the Company's long-term debt is considered to approximate the fair value of such debt for all periods presented based upon the interest rates that the Company believes it can currently obtain for similar debt.
Off-Balance Sheet Arrangements
As of December 31, 2022, the Company had approximately $6,710 of borrowing capacity under the Revolving Credit Facility pledged as collateral to secure outstanding letters of credit, which remained consistent from 2021.
17. OPTIONS AND AWARDS
Stock-based compensation expense consists of stock-based payment awards made to employees and directors, including employee stock options and restricted stock awards, based on estimated fair values. As stock-based compensation expense recognized in the Company’s consolidated statements of income for the years ended December 31, 2022, 2021, and 2020 was based on awards ultimately expected to vest, it has been reduced for estimated forfeitures. The Company estimates forfeitures at the time of grant and, if necessary, revises the estimate in subsequent periods if actual forfeitures differ.
The Company has one active stock incentive plan, the 2022 Omnibus Incentive Plan (the 2022 Plan), which was approved by the Company's stockholders on May 26, 2022, and replaced the Company's prior option plan, the 2017 Omnibus Incentive Plan (the 2017 Plan).
2022 Omnibus Incentive Plan (2022 Plan) — During the second quarter of 2022, the Company's shareholders approved the 2022 Plan. Including the shares rolled over from the 2017 Plan, the 2022 Plan provides for the issuance of 3,452 shares of common stock. The number of shares available to be issued under the 2022 Plan will be reduced by (i) one share for each share that relates to an option or stock appreciation right award and (ii) two shares for each share which relates to an award other than a stock option or stock appreciation right award (a full-value award). Non-employee director options, to the extent granted, will vest and become exercisable in three equal annual installments, or the length of the term if less than three years , on the completion of each year of service measured from the grant date. All other options generally vest over five years at 20 % per year on the anniversary of the grant date. Options expire ten years from the date of grant. At December 31, 2022, the total number of shares available for issuance under the 2022 Plan was 2,861 .
2017 Omnibus Incentive Plan (2017 Plan) — The 2017 Plan provided for the issuance of 6,881 shares of common stock which are to be proportionally adjusted in the event of any Equity Restructuring. The number of shares available to be issued under the 2017 Plan were adjusted to 8,118 shares of common stock in order to reflect the proportional adjustments as part of the spin-off transaction that occurred in October 2019. The number of shares available to be issued under the 2017 Plan will be reduced by (i) one share for each share that relates to an option or stock appreciation right award and (ii) 2.5 shares for each share which relates to an award other than a stock option or stock appreciation right award (a full-value award). Granted non-employee director options vest and become exercisable in three equal annual installments, or the length of the term if less than three years , on the completion of each year of service measured from the grant date. All other options generally vest over five years at 20 % per year on the anniversary of the grant date. Options expire ten years from the date of grant. The Company granted 165 stock options and 116 restricted stock awards from the 2017 Plan in the first half of 2022 prior to the retirement of the 2017 plan.
117
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
The Company uses the Black-Scholes option-pricing model to recognize the value of stock-based compensation expense for stock option awards. Determining the appropriate fair-value model and calculating the fair value of stock option awards at the grant date requires judgment, including estimating stock price volatility, expected option life, and forfeiture rates. The fair-value of the restricted stock awards at the grant date is based on the market price on the grant date, adjusted for forfeiture rates. The Company develops estimates based on historical data and market information, which can change significantly over time. The Black-Scholes model required the Company to make several key judgments including:
•The expected option term is calculated by the average of the contractual term of the options and the weighted average vesting period for all options. The calculation of the expected option term is based on the Company's experience due to sufficient history.
•The Company utilizes its own experience to calculate estimated volatility for options granted.
•The dividend yield is based on the Company's historical pattern of dividends as well as expected dividend patterns.
•The risk-free rate is based on the implied yield of U.S. Treasury notes as of the grant date with a remaining term approximately equal to the expected term.
•Estimated forfeiture rate of approximately 7.84 % per year is based on the Company's historical forfeiture activity of unvested stock options.
Stock Options
The Company granted 581 , 621 and 669 stock options from the available plans during the year ended December 31, 2022, 2021 and 2020, respectively. The Company used the following assumptions for stock options granted during the years ended December 31, 2022, 2021 and 2020:
| Grant Year | Options Granted | Weighted Average Risk-Free Rate | Expected Life | Weighted Average Volatility | Weighted Average Dividend Yield | |||||||||||||||||||||||||||
| 2022 | ||||||||||||||||||||||||||||||||
| 2021 | ||||||||||||||||||||||||||||||||
| 2020 | ||||||||||||||||||||||||||||||||
For the years ended December 31, 2022, 2021 and 2020, the following represents the exercise price and fair value displayed at grant date for stock option grants:
| Grant Year | Granted | Weighted Average Exercise Price | Weighted Average Fair Value of Options | |||||||||||||||||
| 2022 | $ | $ | ||||||||||||||||||
| 2021 | $ | $ | ||||||||||||||||||
| 2020 | $ | $ | ||||||||||||||||||
The weighted average exercise price equaled the weighted average fair value of common stock on the grant date for all options granted during the periods ended December 31, 2022, 2021 and 2020 and therefore, the intrinsic value was $0
118
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
The following table represents the employee stock option activity during the year ended December 31, 2022, 2021 and 2020:
| Number of Options Outstanding | Weighted Average Exercise Price | Number of Options Vested | Weighted Average Exercise Price of Options Vested | ||||||||||||||||||||
| January 1, 2020 | $ | $ | |||||||||||||||||||||
| Granted | |||||||||||||||||||||||
| Forfeited | ( | ||||||||||||||||||||||
| Exercised | ( | ||||||||||||||||||||||
| December 31, 2020 | $ | $ | |||||||||||||||||||||
| Granted | |||||||||||||||||||||||
| Forfeited | ( | ||||||||||||||||||||||
| Exercised | ( | ||||||||||||||||||||||
| December 31, 2021 | $ | $ | |||||||||||||||||||||
| Granted | — | — | |||||||||||||||||||||
| Forfeited | ( | — | — | ||||||||||||||||||||
| Exercised | ( | — | — | ||||||||||||||||||||
| December 31, 2022 | $ | $ | |||||||||||||||||||||
The following summary information reflects stock options outstanding, vested and related details as of December 31, 2022:
| Stock Options Outstanding | Stock Options Vested | |||||||||||||||||||||||||||||||||||||
| Number Outstanding | Black-Scholes Fair Value | Remaining Contractual Life (Years) | Vested and Exercisable | |||||||||||||||||||||||||||||||||||
| Year of Grant | Exercise Price | |||||||||||||||||||||||||||||||||||||
| 2013 | - | |||||||||||||||||||||||||||||||||||||
| 2014 | - | |||||||||||||||||||||||||||||||||||||
| 2015 | - | |||||||||||||||||||||||||||||||||||||
| 2016 | - | |||||||||||||||||||||||||||||||||||||
| 2017 | - | |||||||||||||||||||||||||||||||||||||
| 2018 | - | |||||||||||||||||||||||||||||||||||||
| 2019 | - | |||||||||||||||||||||||||||||||||||||
| 2020 | - | |||||||||||||||||||||||||||||||||||||
| 2021 | - | |||||||||||||||||||||||||||||||||||||
| 2022 | $ | $ | ||||||||||||||||||||||||||||||||||||
| TOTAL | $ | |||||||||||||||||||||||||||||||||||||
The aggregate intrinsic value of options outstanding, vested and expected to vest as of December 31, 2022, 2021 and 2020 is as follows:
| December 31, | ||||||||||||||||||||
| Options | 2022 | 2021 | 2020 | |||||||||||||||||
| Outstanding | $ | $ | $ | |||||||||||||||||
| Vested | ||||||||||||||||||||
| Expected to vest | ||||||||||||||||||||
The intrinsic value is calculated as the difference between the market value of the underlying common stock and the exercise price of the options. The aggregate intrinsic value of options that vested during the year ended December 31, 2022, 2021 and 2020 was $27,955 , $27,731 , and $26,030 , respectively. The total intrinsic value of options exercised during the year ended December 31, 2022, 2021 and 2020 was $47,441 , $34,278 , and $45,081 , respectively.
119
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Restricted Stock Awards
The Company granted 233 , 222 and 281 restricted stock awards during the years ended December 31, 2022, 2021 and 2020, respectively. All awards were granted at an issue price of $0 and generally vest over five years . The fair value per share of restricted awards granted during the years ended December 31, 2022, 2021 and 2020 ranged from $73.17 to $94.88 , $72.84 to $93.31 and $35.47 to $58.06 , respectively. The fair value per share includes quarterly stock awards to non-employee directors.
A summary of the status of the Company's non-vested restricted stock awards as of December 31, 2022 and changes during the years ended December 31, 2022, 2021 and 2020 is presented below:
| Non-Vested Restricted Awards | Weighted Average Grant Date Fair Value | ||||||||||
| Nonvested at January 1, 2020 | $ | ||||||||||
| Granted | |||||||||||
| Vested | ( | ||||||||||
| Forfeited | ( | ||||||||||
| Nonvested at December 31, 2020 | $ | ||||||||||
| Granted | |||||||||||
| Vested | ( | ||||||||||
| Forfeited | ( | ||||||||||
| Nonvested at December 31, 2021 | $ | ||||||||||
| Granted | |||||||||||
| Vested | ( | ||||||||||
| Forfeited | ( | ||||||||||
| Nonvested at December 31, 2022 | $ | ||||||||||
During the year ended December 31, 2022, the Company granted 18 automatic quarterly stock awards to non-employee directors for their service on the Company's board of directors from the 2017 and 2022 Plan. The fair value per share of these stock awards ranged from $75.33 to $86.34 based on the market price on the grant date.
Long-Term Incentive Plan
On August 27, 2019, the Board approved the Long-Term Incentive Plan (the 2019 LTI Plan). The 2019 LTI Plan provides that certain employees of the Company who assisted in the consummation of the spin-off transaction in 2019 are granted shares of restricted stock upon successful completion. The 2019 LTI Plan provides for the issuance of 500 shares of Pennant restricted stock. The shares are vested over five years at 20 % per year on the anniversary of the grant date. If a recipient is terminated or voluntarily leaves the Company, all shares subject to restriction or not yet vested shall be entirely forfeited. The total stock-based compensation related to the 2019 LTI Plan was approximately $836 , $854 , and $881 for the years ended December 31, 2022, 2021 and 2020, respectively.
Stock-based compensation expense recognized for the Company's equity incentive plans and long-term incentive plan for the years ended December 31, 2022, 2021, and 2020 was as follows:
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
| Stock-based compensation expense related to stock options | $ | $ | $ | ||||||||||||||
| Stock-based compensation expense related to restricted stock awards | |||||||||||||||||
| Stock-based compensation expense related to stock options and restricted stock awards to non-employee directors | |||||||||||||||||
| TOTAL | $ | $ | $ | ||||||||||||||
120
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
18. LEASES
The Company leases from CareTrust REIT, Inc. (CareTrust) real property associated with 97 affiliated skilled nursing and senior living facilities used in the Company’s operations, 96 of which are under nine “triple-net” master lease agreements (collectively, the Master Leases), which range in terms from 13 to 20 years. At the Company’s option, the Master Leases may be extended for two or three five-year renewal terms beyond the initial term, on the same terms and conditions. The extension of the term of any of the Master Leases is subject to the following conditions: (1) no event of default under any of the Master Leases having occurred and being continuing; and (2) the tenants providing timely notice of their intent to renew. The term of the Master Leases is subject to termination prior to the expiration of the current term upon default by the tenants in their obligations, if not cured within any applicable cure periods set forth in the Master Leases. If the Company elects to renew the term of a Master Lease, the renewal will be effective to all, but not less than all, of the leased property then subject to the Master Lease. Additionally, four of the 97 facilities leased from CareTrust include an option to purchase that the Company can exercise starting on December 1, 2024.
The Company does not have the ability to terminate the obligations under a Master Lease prior to its expiration without CareTrust’s consent. If a Master Lease is terminated prior to its expiration other than with CareTrust’s consent, the Company may be liable for damages and incur charges such as continued payment of rent through the end of the lease term as well as maintenance and repair costs for the leased property.
The rent structure under the Master Leases includes a fixed component, subject to annual escalation equal to the lesser of (1) the percentage change in the Consumer Price Index (but not less than zero ) or (2) 2.5 %. In addition to rent, the Company is required to pay the following: (1) all impositions and taxes levied on or with respect to the leased properties (other than taxes on the income of the lessor); (2) all utilities and other services necessary or appropriate for the leased properties and the business conducted on the leased properties; (3) all insurance required in connection with the leased properties and the business conducted on the leased properties; (4) all facility maintenance and repair costs; and (5) all fees in connection with any licenses or authorizations necessary or appropriate for the leased properties and the business conducted on the leased properties. The terms and conditions of the one stand-alone lease are substantially the same as those for the master leases described above. Total rent expense for continuing operations under the Master Leases was approximately $64,178 , $59,571 and $52,838 for the years ended December 31, 2022, 2021 and 2020, respectively.
Among other things, under the Master Leases, the Company must maintain compliance with specified financial covenants measured on a quarterly basis, including a portfolio coverage ratio and a minimum rent coverage ratio. The Master Leases also include certain reporting, legal and authorization requirements. The Company is in compliance with requirements of the Master Leases as of December 31, 2022.
In connection with the spin-off transaction in 2019, the Company guaranteed certain leases of Pennant based on the underlying terms of the leases. The Company does not consider these guarantees to be probable and the likelihood of Pennant defaulting is remote, and therefore no liabilities have been accrued.
The Company leases certain affiliated operations and certain administrative offices under non-cancelable operating leases, most of which have initial lease terms ranging from to 20 years. In addition, the Company leases certain of its equipment under non-cancelable operating leases with initial terms ranging from to five years . Most of these leases contain renewal options, certain of which involve rent increases. Total rent expense for continuing operations inclusive of straight-line rent adjustments and rent associated with the Master Leases noted above, was $153,174 , $139,458 and $129,990 for the year ended December 31, 2022, 2021 and 2020, respectively.
121
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
During 2022, Standard Bearer acquired the real estate of three skilled nursing operations, which were previously under separate long-term lease arrangements. The aggregate reduction in the carrying value of the Company's lease liabilities and right-of-use assets related to this acquisition is $10,080 .
The components of operating lease expense are as follows:
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
Rent - cost of services(1) | $ | $ | $ | ||||||||||||||
| General and administrative expense | |||||||||||||||||
Depreciation and amortization(2) | |||||||||||||||||
Variable lease costs(3) | |||||||||||||||||
| $ | $ | $ | |||||||||||||||
(1)Rent- cost of services includes deferred rent expense adjustments of $493 , $485 and $451 for the years ended December 31, 2022, 2021 and 2020, respectively. Additionally, rent- cost of services includes other variable lease costs such as consumer price index increases and short-term leases of $5,878 , $3,702 , $2,394 for the years ended December 31, 2022, 2021, and 2020 respectively.
(2)Depreciation and amortization is related to the amortization of favorable and direct lease costs.
(3)Variable lease costs, including property taxes and insurance, are classified in cost of services in the Company's consolidated statements of income.
Future minimum lease payments for all leases as of December 31, 2022 are as follows:
| Year | Amount | |||||||
| 2023 | $ | |||||||
| 2024 | ||||||||
| 2025 | ||||||||
| 2026 | ||||||||
| 2027 | ||||||||
| Thereafter | ||||||||
| TOTAL LEASE PAYMENTS | ||||||||
| Less: present value adjustment | ( | |||||||
| PRESENT VALUE OF TOTAL LEASE LIABILITIES | ||||||||
| Less: current lease liabilities | ( | |||||||
| LONG-TERM OPERATING LEASE LIABILITIES | $ | |||||||
Operating lease liabilities are based on the net present value of the remaining lease payments over the remaining lease term. In determining the present value of lease payments, the Company used its incremental borrowing rate based on the information available at the lease commencement date. As of December 31, 2022 and 2021, the weighted average remaining lease term is 15.0 and 14.8 , respectively, and the weighted average discount rate used to determine the operating lease liabilities is 6.7 % and 7.6 %, respectively.
Subsequent to December 31, 2022, the Company expanded its operations through two separate master lease arrangements for 20 stand-alone skilled nursing operations, of which 17 will be operated by the Company's affiliated operating subsidiaries and the remaining three will be subleased to a third-party operator. The aggregate impact to the carrying value of lease liabilities and right-of-use assets related to the two separate master lease agreements is estimated to be approximately $315,337 .
122
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Lessor Activities
In connection with the spin-off transaction in 2019, Ensign affiliates retained ownership of the real estate at 29 senior living operations that were contributed to Pennant. As of December 31, 2022, Ensign affiliates retained ownership of the real estate for these 29 senior living communities. All of these properties are leased to Pennant on a triple-net basis, whereas the respective Pennant affiliates are responsible for all costs at the properties including: (1) all impositions and taxes levied on or with respect to the leased properties (other than taxes on the income of the lessor); (2) all utilities and other services necessary or appropriate for the leased properties and the business conducted on the leased properties; (3) all insurance required in connection with the leased properties and the business conducted on the leased properties; (4) all facility maintenance and repair costs; and (5) all fees in connection with any licenses or authorizations necessary or appropriate for the leased properties and the business conducted on the leased properties. The initial terms range between 14 to 16 years.
Total rental income from all third-party sources for the years ended December 31, 2022, 2021, and 2020 is as follows:
| Year Ended December 31, | |||||||||||||||||
| 2022 | 2021 | 2020 | |||||||||||||||
Pennant(1) | $ | $ | $ | ||||||||||||||
| Other third-party | |||||||||||||||||
| $ | $ | $ | |||||||||||||||
(1) Pennant rental income includes variable rent such as property taxes of $1,318 , $1,199 , and $1,224 during the year ended December 31, 2022, 2021, and 2020.
Future annual rental income for all leases as of December 31, 2022 were as follows:
| Year | Amount(1) | |||||||
| 2023 | $ | |||||||
| 2024 | ||||||||
| 2025 | ||||||||
| 2026 | ||||||||
| 2027 | ||||||||
| Thereafter | ||||||||
| TOTAL | $ | |||||||
19. SELF INSURANCE LIABILITIES
The following table represents activity in our insurance liabilities as of and for the years ended December 31, 2022 and 2021:
| Amount | ||||||||
Balance January 1, 2021 | $ | |||||||
| Current year provisions | ||||||||
| Claims paid and direct expenses | ( | |||||||
| Change in long-term insurance losses recoverable | ( | |||||||
Balance December 31, 2021 | $ | |||||||
| Current year provisions | ||||||||
| Claims paid and direct expenses | ( | |||||||
| Change in long-term insurance losses recoverable | ||||||||
Balance December 31, 2022 | $ | |||||||
123
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
20. DEFINED CONTRIBUTION PLANS
The Company has a 401(k) defined contribution plan (the 401(k) Plan), whereby eligible employees may contribute up to 90 % of their annual basic earnings, subject to applicable annual Internal Revenue Code limits. Additionally, the 401(k) Plan provides for discretionary matching contributions (as defined in the 401(k) Plan) by the Company. The Company expensed matching contributions to the 401(k) Plan of $2,418 , $2,121 , and $1,889 during the years ended December 31, 2022, 2021 and 2020, respectively.
During the year ended December 31, 2019, the Company implemented non-qualified deferred compensation plan (the DCP) that was effective in 2019 for certain executives. The plan was then offered to other highly compensated employees, which went into effect on January 1, 2020. These individuals are otherwise ineligible for participation in the Company's 401(k) plan. The DCP allows participating employees to defer the receipt of a portion of their base compensation and certain employees up to 100 % of their eligible bonuses. Additionally, the plan allows for the employee deferrals to be deposited into a rabbi trust and the funds are generally invested in individual variable life insurance contracts owned by the Company that are specifically designed to informally fund savings plans of this nature. The Company paid for related administrative costs, which were not significant during fiscal years 2022, 2021 and 2020.
As of the years ended December 31, 2022, 2021, and 2020, the Company accrued $33,017 , $26,832 and $14,232 , respectively, as long term deferred compensation in other long term liabilities on the consolidated balance sheet. Cash surrender value of the contracts is based on investment funds that shadow the investment allocations specified by participants in the deferred compensation plan. Refer to Note 6, Fair Value Measurements for more information on the funds.
For the year ended December 31, 2022, the Company recorded a loss on the investment acquired in connection with our deferred compensation plan of $4,188 , which is included in other income (expense), net. During the same period, the Company recorded an offsetting reduction in expense of $4,051 , which is allocated between cost of services and general and administrative expenses.
21. COMMITMENTS AND CONTINGENCIES
Regulatory Matters — Laws and regulations governing Medicare and Medicaid programs are complex and subject to review and interpretation. Compliance with such laws and regulations is evaluated regularly, the results of which can be subject to future governmental review and interpretation, and can include significant regulatory action including fines, penalties, and exclusion from certain governmental programs. Included in these laws and regulations is monitoring performed by the Office of Civil Rights which covers the Health Insurance Portability and Accountability Act of 1996, the terms of which require healthcare providers (among other things) to safeguard the privacy and security of certain patient protected health information.
Cost-Containment Measures — Both government and private pay sources have instituted cost-containment measures designed to limit payments made to providers of healthcare services, and there can be no assurance that future measures designed to limit payments made to providers will not adversely affect the Company.
124
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
Indemnities — From time to time, the Company enters into certain types of contracts that contingently require the Company to indemnify parties against third-party claims. These contracts primarily include (i) certain real estate leases, under which the Company may be required to indemnify property owners or prior facility operators for post-transfer environmental obligations or other liabilities and other claims arising from the Company’s use of the applicable premises, (ii) operations transfer agreements, in which the Company agrees to indemnify past operators of facilities the Company acquires against certain liabilities arising from the transfer of the operation and/or the operation thereof after the transfer to the Company's independent operating subsidiary, (iii) certain lending agreements, under which the Company may be required to indemnify the lender against various claims and liabilities, and (iv) certain agreements with the Company’s officers, directors and others, under which the Company may be required to indemnify such persons for liabilities arising out of the nature of their relationship to the Company. The terms of such obligations vary by contract and, in most instances, do not expressly state or include a specific or maximum dollar amount. Generally, amounts under these contracts cannot be reasonably estimated until a specific claim is asserted. Consequently, because no claims have been asserted, no liabilities have been recorded for these obligations on the Company’s consolidated balance sheets for any of the periods presented.
In connection with the spin-off transaction in 2019, certain landlords required, in exchange for their consent to the transaction, that the Company's lease guarantees remain in place for a certain period of time following the transaction. These guarantees could result in significant additional liabilities and obligations for the Company if Pennant were to default on their obligations under their leases with respect to these properties.
U.S. Department of Justice Civil Investigative Demand — On May 31, 2018, the Company received a Civil Investigative Demand (CID) from the U.S. Department of Justice stating that it was investigating whether there had been a violation of the False Claims Act and/or the Anti-Kickback Statute with respect to relationships between certain of the Company’s independently operated skilled nursing facilities and persons who serve or have served as medical directors, advisory board participants or other potential referral sources. The CID covered the period from October 3, 2013 through 2018, and was limited in scope to ten of the Company’s Southern California independent operating entities. In October 2018, the Department of Justice made an additional request for information covering the period of January 1, 2011 through 2018, relating to the same topic. As a general matter, the Company’s independent operating entities have established and maintain policies and procedures to promote compliance with the False Claims Act, the Anti-Kickback Statute, and other applicable regulatory requirements. The Company fully cooperated with the U.S. Department of Justice and promptly responded to its requests for information; in April 2020, the Company was advised that the U.S. Department of Justice declined to intervene in any subsequent action filed by a relator in connection with the subject matter of this investigation.
U.S. House of Representatives Select Subcommittee Request — In 2020, the U.S. House of Representatives Select Subcommittee on the Coronavirus Crisis launched a nation-wide investigation into the COVID-19 pandemic, which included the impact of the coronavirus on residents and employees in nursing homes. In June 2020, the Company received a document and information request from the House Select Subcommittee in connection with its investigation. The Company has cooperated in responding to this inquiry. In July 2022 and thereafter, the Company received follow up requests for additional documents and information. The Company has responded to these requests, and continued to cooperate with the House Select Subcommittee in connection with its investigation. On December 9, 2022, the House Select Subcommittee issued its final report summarizing its investigation and related recommendations designed "to strengthen the nation's ability to prevent and respond to public health and economic emergencies." According to the information provided by the House Select Subcommittee, the issuance of this report was the House Select Subcommittee's final official act.
Litigation — The skilled nursing business involves a significant risk of liability given the age and health of the patients and residents served by the Company's independent operating subsidiaries. The Company, its independent operating subsidiaries, and others in the industry are subject to an increasing number of claims and lawsuits, including professional liability claims, alleging that services provided have resulted in personal injury, elder abuse, wrongful death or other related claims. In addition, the Company, its independent operating subsidiaries, and others in the industry are subject to claims and lawsuits in connection with COVID-19 and a facility's preparation for and/or response to COVID-19. The defense of these lawsuits may result in significant legal costs, regardless of the outcome, and can result in large settlement amounts or damage awards.
125
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
In addition to the potential lawsuits and claims described above, the Company and its independent operating subsidiaries are also subject to potential lawsuits under the Federal False Claims Act and comparable state laws alleging submission of fraudulent claims for services to any healthcare program (such as Medicare or Medicaid) or other payor. A violation may provide the basis for exclusion from Federally-funded healthcare programs. Such exclusions could have a correlative negative impact on the Company’s financial performance. Under the qui tam or "whistleblower" provisions of the False Claims Act, a private individual with knowledge of fraud or potential fraud may bring a claim on behalf of the Federal Government and receive a percentage of the Federal Government's recovery. Due to these whistleblower incentives, qui tam lawsuits have become more frequent. For example, and despite the decision of the U.S. Department of Justice to decline to participate in litigation based on the subject matter of its previously issued Civil Investigative Demand, the involved qui tam relator has continued on with the lawsuit and is pursuing claims that the Company and certain of its independent operating subsidiaries have allegedly violated the False Claims Act and/or the Anti-Kickback Statute (AKS).
In addition to the Federal False Claims Act, some states, including California, Arizona and Texas, have enacted similar whistleblower and false claims laws and regulations. Further, the Deficit Reduction Act of 2005 created incentives for states to enact anti-fraud legislation modeled on the Federal False Claims Act. As such, the Company and its independent operating subsidiaries could face increased scrutiny, potential liability and legal expenses and costs based on claims under state false claims acts in markets in which its independent operating subsidiaries do business.
In May 2009, Congress passed the Fraud Enforcement and Recovery Act (FERA) which made significant changes to the Federal False Claims Act and expanded the types of activities subject to prosecution and whistleblower liability. Following changes by FERA, health care providers face significant penalties for the knowing retention of government overpayments, even if no false claim was involved. Health care providers can now be liable for knowingly and improperly avoiding or decreasing an obligation to pay money or property to the government. This includes the retention of any government overpayment. The government can argue, therefore, that a Federal False Claims Act violation can occur without any affirmative fraudulent action or statement, as long as the action or statement is knowingly improper. In addition, FERA extended protections against retaliation for whistleblowers, including protections not only for employees, but also contractors and agents. Thus, an employment relationship is generally not required in order to qualify for protection against retaliation for whistleblowing.
Healthcare litigation (including class action litigation) is common and is filed based upon a wide variety of claims and theories, and the Company's independent operating subsidiaries are routinely subjected to varying types of claims, including class action "staffing" suits where the allegation is understaffing at the facility level. These class-action “staffing” suits have the potential to result in large jury verdicts and settlements, and may result in significant legal costs. The Company expects the plaintiffs' bar to continue to be aggressive in their pursuit of these staffing and similar claims. While the Company has been able to settle these claims without an ongoing material adverse effect on its business, future claims could be brought that may materially affect its business, financial condition and results of operations.
Other claims and suits, including class actions, continue to be filed against the Company and other companies in its industry. The Company and its independent operating subsidiaries have been subjected to, and are currently involved in, class action litigation alleging violations (alone or in combination) of state and federal wage and hour laws as related to the alleged failure to pay wages, to timely provide and authorize meal and rest breaks, and related causes of action. The Company does not believe that the ultimate resolution of these actions will have an ongoing material adverse effect on the Company’s business, cash flows, financial condition or results of operations.
The Company and its independent operating subsidiaries have been, and continue to be, subject to claims, findings and legal actions that arise in the ordinary course of the various businesses, including healthcare and non-healthcare services. These claims include, but are not limited to, potential claims filed by residents, customers, patients and responsible parties related to patient care and treatment (professional negligence claims); to non-care based activities of certain of the subsidiaries; and to employment related claims filed by current or former employees. A significant increase in the number of these claims, or an increase in the amounts owing should plaintiffs be successful in their prosecution of these claims, could materially adversely affect the Company’s business, financial condition, results of operations and cash flows. In addition, these claims could impact the Company's ability to procure insurance to cover its exposure related to the various services provided by its independent operating subsidiaries to their residents, customers and patients.
126
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
The Company and its independent subsidiaries are also subject to requests for information and investigations by other State and Federal governmental entities (e.g., offices of the attorney general and offices of the inspector general). The Company cannot predict or provide any assurance as to the possible outcome of any inquiry, investigation or litigation. If any such inquiry, investigation or litigation were to proceed, and the Company and its independent operating subsidiaries are subjected to, alleged to be liable for, or agree to a settlement of, claims or obligations under Federal Medicare statutes, the Federal False Claims Act, or similar state and federal statutes and related regulations, or if the Company or its independent operating subsidiaries are alleged or found to be liable on theories of general or professional negligence or wage and hour violations, the Company's business, financial condition and results of operations and cash flows could be materially and adversely affected and its stock price could be adversely impacted. Among other things, any settlement or litigation could involve the payment of substantial sums to settle any alleged violations, and may also include the assumption of specific procedural and financial obligations by the Company or its independent operating subsidiaries under a corporate integrity agreement and/or other such arrangement.
Medicare Revenue Recoupments — The Company's independent operating entities are subject to regulatory reviews relating to the provision of Medicare services, billings and potential overpayments as a result of Recovery Audit Contractors (RAC), Program Safeguard Contractors, and Medicaid Integrity Contractors programs (collectively referred to as Reviews). For several months during the COVID-19 pandemic, the Centers for Medicare and Medicaid Services (CMS) suspended its Targeted Probe and Educate Program. Beginning in August 2020, CMS resumed Targeted Probe and Educate Program activity. If an operation fails a Review and/or subsequent Reviews, the operation could then be subject to extended review or an extrapolation of the identified error rate to billings in the same time period. The Company anticipates that these Reviews could increase in frequency in the future. As of December 31, 2022 and since, 34 of the Company's independent operating subsidiaries had Reviews scheduled, on appeal, or in a dispute resolution process.
Concentrations
Credit Risk — The Company has significant accounts receivable balances, the collectability of which is dependent on the availability of funds from certain governmental programs, primarily Medicare and Medicaid. These receivables represent the only significant concentration of credit risk for the Company. The Company does not believe there are significant credit risks associated with these governmental programs. The Company believes that an appropriate allowance has been recorded for the possibility of these receivables proving uncollectible, and continually monitors and adjusts these allowances as necessary. The Company’s receivables from Medicare and Medicaid payor programs accounted for 56.3 % and 54.0 % of its total accounts receivable as of December 31, 2022 and 2021, respectively. Revenue from reimbursement under the Medicare and Medicaid programs accounted for 73.7 %, 73.6 % and 74.5 % of the Company's revenue for the years ended December 31, 2022, 2021 and 2020, respectively.
Cash in Excess of FDIC Limits — The Company currently has bank deposits with financial institutions in the U.S. that exceed FDIC insurance limits. FDIC insurance provides protection for bank deposits up to $250. In addition, the Company has uninsured bank deposits with a financial institution outside the U.S. As of January 30, 2023, the Company's uninsured cash deposits are not material. All uninsured bank deposits are held at high quality credit institutions.
22. COMMON STOCK REPURCHASE PROGRAM
On July 28, 2022, the Board of Directors approved a stock repurchase program pursuant to which the Company may repurchase up to $20,000 of its common stock under the program for a period of approximately 12 months from August 2, 2022. Under this program, the Company is authorized to repurchase its issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. The Company did not purchase any shares pursuant to this stock repurchase program in the year ended December 31, 2022. The share repurchase program does not obligate the Company to acquire any specific number of shares.
On February 9, 2022, the Board of Directors approved a stock repurchase program pursuant to which the Company could repurchase up to $20,000 of its common stock under the program for a period of approximately 12 months from February 10, 2022. Under this program, the Company was authorized to repurchase its issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. During the three months ended June 30, 2022, the Company repurchased 271 shares of its common stock for $20,000 . This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
127
| THE ENSIGN GROUP, INC. | ||||||||
NOTES TO THE CONSOLIDATED FINANCIAL STATEMENTS - (Continued) | ||||||||
On October 21, 2021, the Board of Directors approved a stock repurchase program pursuant to which the Company could repurchase up to $20,000 of its common stock under the program for a period of approximately 12 months that started on October 29, 2021. Under this program, the Company was authorized to repurchase its issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. The Company repurchased 133 and 132 shares of its common stock for $9,882 and $10,118 during the years ended December 31, 2022 and 2021, respectively. This repurchase program expired upon the repurchase of the fully authorized amount under the plan and is no longer in effect.
On March 4, 2020 and March 13, 2020, the Board of Directors approved two stock repurchase programs pursuant to which the Company was authorized to repurchase up to $20,000 and $5,000 , respectively, of its common stock under the programs for a period of approximately 12 months. Under these programs, the Company was authorized to repurchase its issued and outstanding common shares from time to time in open-market and privately negotiated transactions and block trades in accordance with federal securities laws. During the first quarter of 2020, the Company repurchased 503 and 189 shares of its common stock for $20,000 and $5,000 , respectively. These repurchase programs expired upon the repurchase of the full authorized amount under the two plans and are no longer in effect.
Item 9. CHANGES IN AND DISAGREEMENTS WITH ACCOUNTANTS ON ACCOUNTING AND FINANCIAL DISCLOSURES
None.
Item 9A. CONTROLS AND PROCEDURES
(a) Conclusion Regarding the Effectiveness of Disclosure Controls and Procedures
The Company maintains disclosure controls and procedures that are designed to ensure that information we are required to disclose in reports that we file or submit under the Exchange Act is recorded, processed, summarized and reported within the time periods specified in Securities and Exchange Commission rules and forms. Disclosure controls and procedures include, without limitation, controls and procedures designed to ensure that information required to be disclosed by a company in the reports that it files or submits under the Exchange Act is accumulated and communicated to its management, including its principal executive and principal financial officers, or persons performing similar functions, as appropriate to allow timely decisions regarding required disclosure. In designing and evaluating our disclosure controls and procedures, our management recognized that any system of controls and procedures, no matter how well designed and operated, can provide only reasonable assurance of achieving the desired control objectives, as ours are designed to do, and management necessarily was required to apply its judgment in evaluating the cost-benefit relationship of possible controls and procedures.
In connection with the preparation of this Annual Report on Form 10-K our management evaluated, with the participation of our Chief Executive Officer and our Chief Financial Officer, the effectiveness of our disclosure controls and procedures, as such term is defined under Rule 13a-15(e) promulgated under the Exchange Act. Based on this evaluation, our Chief Executive Officer and our Chief Financial Officer have concluded that our disclosure controls and procedures were effective as of the end of the period covered by this Annual Report on Form 10-K.
(b) Management's Report on Internal Control over Financial Reporting
Our management is responsible for establishing and maintaining adequate internal control over financial reporting, as defined in Rule 13a-15(f) promulgated under the Exchange Act. Internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
Our management, with the participation of our Chief Executive Officer and our Chief Financial Officer, evaluated the effectiveness of our internal control over financial reporting using the criteria set forth by the Committee of Sponsoring Organizations of the Treadway Commission in Internal Control - Integrated Framework (2013). As a result of this assessment, management concluded that, as of December 31, 2022, our internal control over financial reporting was effective in providing reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles.
Our independent registered public accounting firm, Deloitte & Touche LLP, has audited the consolidated financial statements included in this Annual Report on Form 10-K and, as part of their audit, has issued an audit report, included herein, on the effectiveness of our internal control over financial reporting. Their report is set forth below.
(c) Changes in Internal Control over Financial Reporting
There were no changes in our internal control over financial reporting, as defined in Rule 13a-15(f) promulgated under the Exchange Act, that occurred during the fourth quarter of fiscal 2022 that have materially affected, or are reasonably likely to materially affect, our internal control over financial reporting.
(d) Report of Independent Registered Public Accounting Firm
To the Stockholders and the Board of Directors of
The Ensign Group, Inc.
San Juan Capistrano, California
Opinion on Internal Control over Financial Reporting
We have audited the internal control over financial reporting of The Ensign Group, Inc. and subsidiaries (the “Company”) as of December 31, 2022, based on criteria established in Internal Control — Integrated Framework (2013) issued by the Committee of Sponsoring Organizations of the Treadway Commission (COSO). In our opinion, the Company maintained, in all material respects, effective internal control over financial reporting as of December 31, 2022, based on criteria established in Internal Control — Integrated Framework (2013) issued by COSO.
We have also audited, in accordance with the standards of the Public Company Accounting Oversight Board (United States) (PCAOB), the consolidated financial statements as of and for the year ended December 31, 2022 of the Company and our report dated February 2, 2023, expressed an unqualified opinion on those financial statements.
Basis for Opinion
The Company’s management is responsible for maintaining effective internal control over financial reporting and for its assessment of the effectiveness of internal control over financial reporting, included in the accompanying Management’s Report on Internal Control over Financial Reporting. Our responsibility is to express an opinion on the Company’s internal control over financial reporting based on our audit. We are a public accounting firm registered with the PCAOB and are required to be independent with respect to the Company in accordance with the U.S. federal securities laws and the applicable rules and regulations of the Securities and Exchange Commission and the PCAOB.
We conducted our audit in accordance with the standards of the PCAOB. Those standards require that we plan and perform the audit to obtain reasonable assurance about whether effective internal control over financial reporting was maintained in all material respects. Our audit included obtaining an understanding of internal control over financial reporting, assessing the risk that a material weakness exists, testing and evaluating the design and operating effectiveness of internal control based on the assessed risk, and performing such other procedures as we considered necessary in the circumstances. We believe that our audit provides a reasonable basis for our opinion.
Definition and Limitations of Internal Control over Financial Reporting
A company’s internal control over financial reporting is a process designed to provide reasonable assurance regarding the reliability of financial reporting and the preparation of financial statements for external purposes in accordance with generally accepted accounting principles. A company’s internal control over financial reporting includes those policies and procedures that (1) pertain to the maintenance of records that, in reasonable detail, accurately and fairly reflect the transactions and dispositions of the assets of the company; (2) provide reasonable assurance that transactions are recorded as necessary to permit preparation of financial statements in accordance with generally accepted accounting principles, and that receipts and expenditures of the company are being made only in accordance with authorizations of management and directors of the company; and (3) provide reasonable assurance regarding prevention or timely detection of unauthorized acquisition, use, or disposition of the company’s assets that could have a material effect on the financial statements.
Because of its inherent limitations, internal control over financial reporting may not prevent or detect misstatements. Also, projections of any evaluation of effectiveness to future periods are subject to the risk that controls may become inadequate because of changes in conditions, or that the degree of compliance with the policies or procedures may deteriorate.
/s/ DELOITTE & TOUCHE LLP
Costa Mesa, California February 2, 2023
Item 9B. OTHER INFORMATION
None.
Item 9C. DISCLOSURE REGARDING FOREIGN JURISDICTIONS THAT PREVENT INSPECTIONS
Not applicable.
PART III.
Item 10. DIRECTORS, EXECUTIVE OFFICERS AND CORPORATE GOVERNANCE
The information required by this Item is hereby incorporated by reference to our definitive proxy statement for the 2023 Annual Meeting of Stockholders.
We have adopted a code of ethics and business conduct that applies to all employees, including our Chief Executive Officer (our principal executive officer) and Chief Financial Officer (our principal financial officer), and employees of our subsidiaries, as well as each member of our Board of Directors. The code of ethics and business conduct is available on our website at www.ensigngroup.net under the Investor Relations section. The information contained in, or that can be accessed through, our website does not constitute a part of this Annual Report on Form 10-K. We intend to satisfy any disclosure requirement under Item 5.05 of Form 8-K regarding an amendment to, or waiver from, a provision of the code of ethics by posting such information on our website, at the address specified above.
Item 11. EXECUTIVE COMPENSATION
The information required by this Item is hereby incorporated by reference to our definitive proxy statement for the 2023 Annual Meeting of Stockholders.
Item 12. SECURITY OWNERSHIP OF CERTAIN BENEFICIAL OWNERS AND MANAGEMENT AND RELATED STOCKHOLDER MATTERS
The information required by this Item is hereby incorporated by reference to our definitive proxy statement for the 2023 Annual Meeting of Stockholders.
Item 13. CERTAIN RELATIONSHIPS AND RELATED TRANSACTIONS AND DIRECTOR INDEPENDENCE
The information required by this Item is hereby incorporated by reference to our definitive proxy statement for the 2023 Annual Meeting of Stockholders.
Item 14. PRINCIPAL ACCOUNTANT FEES AND SERVICES
The information required by this Item is hereby incorporated by reference to our definitive proxy statement for the 2023 Annual Meeting of Stockholders. Our principal accountant is Deloitte & Touche LLP (PCAOB ID No.34 ).
128
PART IV.
Item 15. EXHIBITS, FINANCIAL STATEMENTS AND SCHEDULES
The following documents are filed as a part of this report:
(a) (1) Financial Statements:
The Financial Statements described in Part II. Item 8 and beginning on page 90 are filed as part of this Annual Report on Form 10-K. | ||
(a) (3) Exhibits: The following exhibits are filed or furnished with or incorporated by reference this Annual Report on Form 10-K.
| Exhibit | File | Exhibit | Filing | Filed | ||||||||||||||||||||||||||||||||||
| No. | Exhibit Description* | Form | No. | No. | Date | Herewith | ||||||||||||||||||||||||||||||||
| Fifth Amended and Restated Certificate of Incorporation of The Ensign Group, Inc., filed with the Delaware Secretary of State on November 15, 2007 | 10-Q | 001-33757 | 3.1 | 12/21/2007 | ||||||||||||||||||||||||||||||||||
| Certificate of Amendment to the Fifth Amended and Restated Certificate of Incorporation of The Ensign Group, Inc., filed with the Delaware Secretary of State on February 4, 2020 | 10-K | 001-33757 | 3.2 | 2/5/2020 | ||||||||||||||||||||||||||||||||||
| Amendment to the Amended and Restated Bylaws, dated August 5, 2014 | 8-K | 001-33757 | 3.2 | 8/8/2014 | ||||||||||||||||||||||||||||||||||
| Amended and Restated Bylaws of The Ensign Group, Inc. | 10-Q | 001-33757 | 3.2 | 12/21/2007 | ||||||||||||||||||||||||||||||||||
| Description of the Common stock of The Ensign Group, Inc. | 10-K | 001-33757 | 4.1 | 2/5/2020 | ||||||||||||||||||||||||||||||||||
| Specimen common stock certificate | S-1 | 333-142897 | 4.1 | 10/5/2007 | ||||||||||||||||||||||||||||||||||
| + | The Ensign Group, Inc. 2007 Omnibus Incentive Plan | S-1 | 333-142897 | 10.3 | 10/5/2007 | |||||||||||||||||||||||||||||||||
| + | Amendment to The Ensign Group, Inc. 2007 Omnibus Incentive Plan | 8-K | 001-33757 | 99.2 | 7/28/2009 | |||||||||||||||||||||||||||||||||
| + | Form of 2007 Omnibus Incentive Plan Notice of Grant of Stock Options; and form of Non-Incentive Stock Option Award Terms and Conditions | S-1 | 333-142797 | 10.4 | 10/5/2007 | |||||||||||||||||||||||||||||||||
| + | Form of 2007 Omnibus Incentive Plan Restricted Stock Agreement | S-1 | 333-142897 | 10.5 | 10/5/2007 | |||||||||||||||||||||||||||||||||
| + | Form of Indemnification Agreement entered into between The Ensign Group, Inc. and its directors, officers and certain key employees | S-1 | 333-142897 | 10.6 | 10/5/2007 | |||||||||||||||||||||||||||||||||
| Form of Independent Consulting and Centralized Services Agreement between Ensign Facility Services, Inc. and certain of its subsidiaries | S-1 | 333-142897 | 10.41 | 5/14/2007 | ||||||||||||||||||||||||||||||||||
| Form of Health Insurance Benefit Agreement pursuant to which certain subsidiaries of The Ensign Group, Inc. participate in the Medicare program | S-1 | 333-142897 | 10.48 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
| Form of Medi-Cal Provider Agreement pursuant to which certain subsidiaries of The Ensign Group, Inc. participate in the California Medicaid program | S-1 | 333-142897 | 10.49 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
| Form of Provider Participation Agreement pursuant to which certain subsidiaries of The Ensign Group, Inc. participate in the Arizona Medicaid program | S-1 | 333-142897 | 10.50 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
| Form of Contract to Provide Nursing Facility Services under the Texas Medical Assistance Program pursuant to which certain subsidiaries of The Ensign Group, Inc. participate in the Texas Medicaid program | S-1 | 333-142897 | 10.51 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
129
| Exhibit | File | Exhibit | Filing | Filed | ||||||||||||||||||||||||||||||||||
| No. | Exhibit Description* | Form | No. | No. | Date | Herewith | ||||||||||||||||||||||||||||||||
| Form of Client Service Contract pursuant to which certain subsidiaries of The Ensign Group, Inc. participate in the Washington Medicaid program | S-1 | 333-142897 | 10.52 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
| Form of Provider Agreement for Medicaid and UMAP pursuant to which certain subsidiaries of The Ensign Group, Inc. participate in the Utah Medicaid program | S-1 | 333-142897 | 10.53 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
| Form of Medicaid Provider Agreement pursuant to which a subsidiary of The Ensign Group, Inc. participates in the Idaho Medicaid program | S-1 | 333-142897 | 10.54 | 10/19/2007 | ||||||||||||||||||||||||||||||||||
| Corporate Integrity Agreement between the Office of Inspector General of the Department of Health and Human Services and The Ensign Group, Inc. dated October 1, 2013. | 10-K | 001-33757 | 10.74 | 2/13/2014 | ||||||||||||||||||||||||||||||||||
| Settlement agreement dated October 1, 2013, entered into among the United States of America, acting through the United States Department of Justice and on behalf of the Office of Inspector General ("OIG-HHS") of the Department of Health and Human Services ("HHS") (collectively the "United States") and the Company. | 8-K | 001-33757 | 10.75 | 5/8/2014 | ||||||||||||||||||||||||||||||||||
| Form of Master Lease by and among certain subsidiaries of The Ensign Group, Inc. and certain subsidiaries of CareTrust REIT, Inc. | 8-K | 001-33757 | 10.1 | 6/5/2014 | ||||||||||||||||||||||||||||||||||
| Form of Guaranty of Master Lease by The Ensign Group, Inc. in favor of certain subsidiaries of CareTrust REIT, Inc., as landlords under the Master Leases | 8-K | 001-33757 | 10.2 | 6/5/2014 | ||||||||||||||||||||||||||||||||||
| Amended and Restated Credit Agreement as of February 5, 2016, by and among The Ensign Group, Inc., SunTrust Bank, now known as Truist, as administrative agent, and the lenders party thereto | 8-K | 001-33757 | 10.1 | 2/8/2016 | ||||||||||||||||||||||||||||||||||
| Second Amended Credit Agreement as of July 19, 2016, by and among The Ensign Group, Inc., SunTrust Bank, now known as Truist, as administrative agent, and the lenders party thereto | 8-K | 001-33757 | 10.1 | 7/25/2016 | ||||||||||||||||||||||||||||||||||
| The Ensign Group, Inc. 2017 Omnibus Incentive Plan | DEF 14A | 001-33757 | A | 4/13/2017 | ||||||||||||||||||||||||||||||||||
| Form of 2017 Omnibus Incentive Plan Notice of Grant of Stock Options; and form of Non-Incentive Stock Option Award Terms and Conditions | 10-K | 001-33757 | 10.87 | 2/8/2018 | ||||||||||||||||||||||||||||||||||
| Form of 2017 Omnibus Incentive Plan Restricted Stock Agreement | 10-K | 001-33757 | 10.88 | 2/8/2018 | ||||||||||||||||||||||||||||||||||
| Form of U.S. Department of Housing and Urban Development Healthcare Facility Note and schedule of individual subsidiary loans, by and among The Ensign Group, Inc.'s subsidiaries listed therein and U.S. Department of Housing and Urban Development | 8-K | 001-33757 | 10.1 | 1/3/2018 | ||||||||||||||||||||||||||||||||||
| Form of U.S. Department of Housing and Urban Development Security Instrument/Mortgage/Deed of Trust | 8-K | 001-33757 | 10.2 | 1/3/2018 | ||||||||||||||||||||||||||||||||||
| Third Amended and Restated Credit Agreement, dated as of October 1, 2019, by and among The Ensign Group, Inc., SunTrust Bank, now known as Truist, as administrative agent, and the lenders party thereto | 8-K | 001-33757 | 10.4 | 10/1/2019 | ||||||||||||||||||||||||||||||||||
| Lease Agreement, dated as of October 1, 2019, by and between The Ensign Group, Inc. and The Pennant Group, Inc. | 8-K | 001-33757 | 10.5 | 10/1/2019 | ||||||||||||||||||||||||||||||||||
| + | The Ensign Services, Inc. Deferred Compensation Plan | 10-K | 001-33757 | 10.1 | 2/3/2021 | |||||||||||||||||||||||||||||||||
| + | First Amendment to The Ensign Services, Inc. Deferred Compensation Plan | 10-K | 001-33757 | 10.2 | 2/3/2021 | |||||||||||||||||||||||||||||||||
130
| Exhibit | File | Exhibit | Filing | Filed | ||||||||||||||||||||||||||||||||||
| No. | Exhibit Description* | Form | No. | No. | Date | Herewith | ||||||||||||||||||||||||||||||||
| First Amendment to Third Amended and Restated Credit Agreement, dated as of February 8, 2022, by and among The Ensign Group, Inc., Standard Bearer Healthcare REIT, Inc., Truist Bank (as successor by merger to SunTrust Bank), as administrative agent, and the lenders party thereto | 10-K | 001-33757 | 10.1 | 2/9/2022 | ||||||||||||||||||||||||||||||||||
| Second Amendment to Third Amended and Restated Credit Agreement, dated as of April 8, 2022, by and among The Ensign Group, Inc. and Truist Bank, as administrative agent, and the lenders party thereto. | 8-K | 001-33757 | 10.1 | 4/12/2022 | ||||||||||||||||||||||||||||||||||
| The Ensign Group, Inc. 2022 Omnibus Incentive Plan | DEF 14A | 001-33757 | A | 4/14/2022 | ||||||||||||||||||||||||||||||||||
| Form of 2022 Omnibus Incentive Plan Notice of Grant of Stock Options; and form of Non-Incentive Stock Option Award Terms and Conditions | X | |||||||||||||||||||||||||||||||||||||
| Form of 2022 Omnibus Incentive Plan Restricted Stock Agreement | X | |||||||||||||||||||||||||||||||||||||
| Subsidiaries of The Ensign Group, Inc., as amended | X | |||||||||||||||||||||||||||||||||||||
| Consent of Deloitte & Touche LLP | X | |||||||||||||||||||||||||||||||||||||
| Certification of Chief Executive Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | X | |||||||||||||||||||||||||||||||||||||
| Certification of Chief Financial Officer pursuant to Section 302 of the Sarbanes-Oxley Act of 2002 | X | |||||||||||||||||||||||||||||||||||||
| Certification of Chief Executive Officer pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | X | |||||||||||||||||||||||||||||||||||||
| Certification of Chief Financial Officer pursuant to Section 906 of the Sarbanes-Oxley Act of 2002 | X | |||||||||||||||||||||||||||||||||||||
| 101 | Interactive data file (furnished electronically herewith pursuant to Rule 406T of Regulations S-T) | |||||||||||||||||||||||||||||||||||||
| 104 | Cover Page Interactive Data File (formatted as Inline XBRL and contained in Exhibit 101) | |||||||||||||||||||||||||||||||||||||
| + | Indicates management contract or compensatory plan. | |||||||||||||||||||||||||||||||||||||
| * | Documents not filed herewith are incorporated by reference to the prior filings identified in the table above. | |||||||||||||||||||||||||||||||||||||
Item 16. FORM 10-K SUMMARY
Not applicable
131
SIGNATURES
Pursuant to the requirements of the Securities Exchange Act of 1934, the registrant has duly caused this report to be signed on its behalf by the undersigned thereunto duly authorized.
| THE ENSIGN GROUP, INC. | ||||||||
| February 2, 2023 | BY: | /s/ SUZANNE D. SNAPPER | ||||||
| Suzanne D. Snapper | ||||||||
| Chief Financial Officer, Executive Vice President and Director (Principal Financial Officer and Accounting Officer and Duly Authorized Officer) | ||||||||
Pursuant to the requirements of the Securities Exchange Act of 1934, this Report has been signed below by the following persons on behalf of the Registrant in the capacities and on the dates indicated.
| Signature | Title | Date | ||||||||||||
| /s/ BARRY R. PORT | Chief Executive Officer and Director (principal executive officer) | February 2, 2023 | ||||||||||||
| Barry R. Port | ||||||||||||||
| /s/ SUZANNE D. SNAPPER | Chief Financial Officer, Executive Vice President and Director (principal financial officer and accounting officer and duly authorized officer) | February 2, 2023 | ||||||||||||
| Suzanne D. Snapper | ||||||||||||||
| /s/ CHRISTOPHER R. CHRISTENSEN | Executive Chairman and Chairman of the Board | February 2, 2023 | ||||||||||||
| Christopher R. Christensen | ||||||||||||||
| /s/ ANN S. BLOUIN | Director | February 2, 2023 | ||||||||||||
| Ann S. Blouin | ||||||||||||||
| /s/ SWATI B. ABBOTT | Director | February 2, 2023 | ||||||||||||
| Swati B. Abbott | ||||||||||||||
| /s/ DAREN J. SHAW | Director | February 2, 2023 | ||||||||||||
| Daren J. Shaw | ||||||||||||||
| /s/ JOHN O. AGWUNOBI | Director | February 2, 2023 | ||||||||||||
| John O. Agwunobi | ||||||||||||||
| /s/ BARRY M. SMITH | Director | February 2, 2023 | ||||||||||||
| Barry M. Smith | ||||||||||||||
132
ATTACHMENTS / EXHIBITS
XBRL TAXONOMY EXTENSION SCHEMA DOCUMENT
XBRL TAXONOMY EXTENSION CALCULATION LINKBASE DOCUMENT
XBRL TAXONOMY EXTENSION DEFINITION LINKBASE DOCUMENT
XBRL TAXONOMY EXTENSION LABEL LINKBASE DOCUMENT
Serious News for Serious Traders! Try StreetInsider.com Premium Free!
You May Also Be Interested In
- Companies Can “Superpower” Their Supply Chains at Blue Yonder ICON, the Premier Industry Conference
- Brusque recebe Mirassol na estreia da Série B, fechando a 1ª rodada
- Global Vitamins Market Size Projected to Reach USD 13.39 billion by 2031, growing at a CAGR of 7.67%
Create E-mail Alert Related Categories
SEC FilingsSign up for StreetInsider Free!
Receive full access to all new and archived articles, unlimited portfolio tracking, e-mail alerts, custom newswires and RSS feeds - and more!
